Liver metastases of pancreatic acinar cell carcinoma with marked nuclear atypia and pleomorphism diagnosed by EUS FNA cytology: a case report with emphasis on FNA cytological findings
- PMID: 17196112
- PMCID: PMC1779360
- DOI: 10.1186/1742-6413-3-29
Liver metastases of pancreatic acinar cell carcinoma with marked nuclear atypia and pleomorphism diagnosed by EUS FNA cytology: a case report with emphasis on FNA cytological findings
Abstract
Background: Acinar cell carcinoma of the pancreas is a rare neoplasm. Although this tumor has been well characterized histologically, the morphological patterns in Fine Needle Aspiration Cytology have not been well defined. Unlike ductal adenocarcinomas, endocrine tumors, and solid pseudopapillary tumors of the pancreas with their characteristic FNA cytological features, acinar cell carcinomas pose a particular diagnostic challenge by sharing many cytomorphologic features with endocrine tumors of the pancreas.
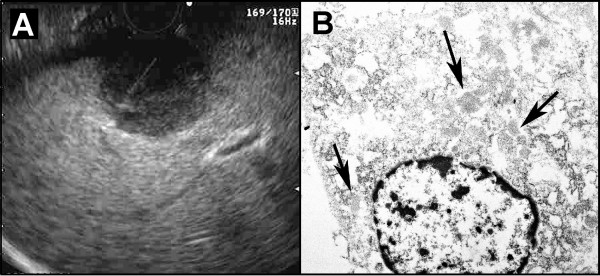
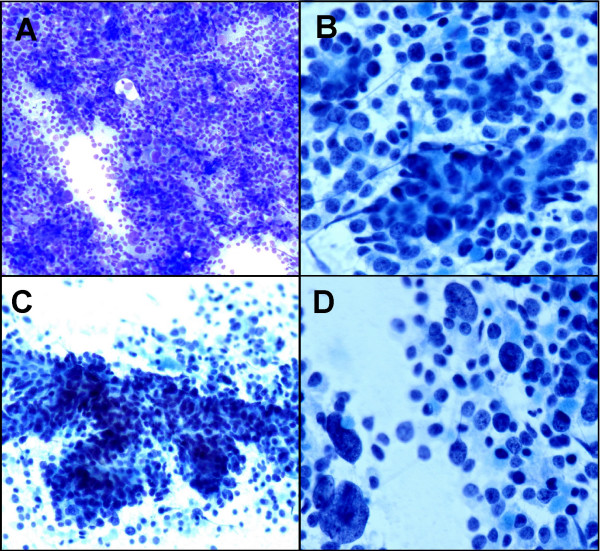
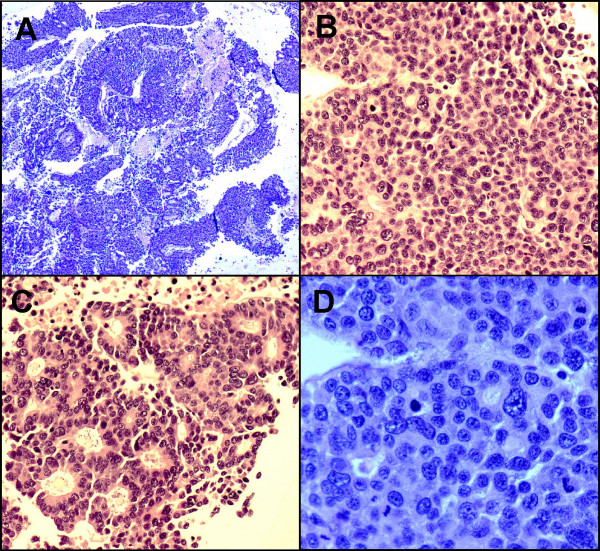
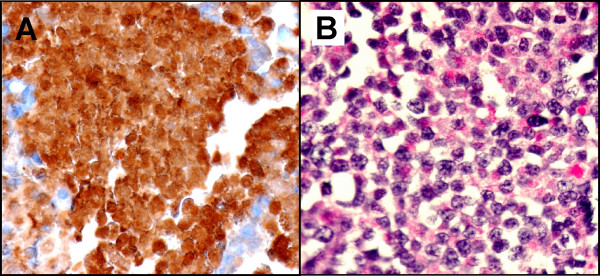
Case presentation: A 37-year-old man presented with lower chest and left upper quadrant abdominal pain. Computed tomography revealed a 7.8 x 7.3 cm irregular, partially cystic mass in the body and tail of the pancreas, and two lesions in the liver compatible with metastases. Subsequently, the patient underwent endoscopic ultrasound-guided fine needle aspiration on one of the two metastatic liver masses. FNA cytology revealed abundant, loosely cohesive clusters of malignant epithelial cells with vaguely acinar and trabecular formations. The pleomorphic nuclei had fine granular chromatin and occasionally small nucleoli. There were scant to moderate amounts of cytoplasm. Scattered, strikingly large tumor cells with giant nuclei, prominent mitoses and associated necrosis were evident. A pancreatic endocrine tumor was suspected initially, but acinar cell carcinoma of the pancreas was confirmed by immunohistochemistry, cytochemical and ultrastructural studies.
Conclusion: We describe a case of pancreatic acinar cell carcinoma with unusual cytomorphologic features mimicking an endocrine tumor of pancreas, encountered in endoscopic ultrasound-guided fine needle aspiration of a metastatic liver mass and discuss the diagnostic approach for this unusual pancreatic tumor in fine needle aspiration cytology.
Figures
References
-
- Bhutani MS, Hawes RH, Baron PL, Sanders-Cliette A, van Velse A, Osborne JF, Hoffman BJ. Endoscopic ultrasound-guided fine needle aspiration of malignant pancreatic lesions. Endoscopy. 1997;29:854–858. - PubMed
-
- Afify AM, al-Khafaji BM, Kim B, Scheiman JM. Endoscopic ultrasound-guided fine needle aspiration of the pancreas. Diagnostic utility and accuracy. Acta Cytol. 2003;47:341–348. - PubMed
LinkOut - more resources
Full Text Sources