

Operative strategies for diverticular peritonitis: a decision analysis between primary resection and anastomosis versus Hartmann's procedures
- PMID: 17197971
- PMCID: PMC1867925
- DOI: 10.1097/01.sla.0000225357.82218.ce
Operative strategies for diverticular peritonitis: a decision analysis between primary resection and anastomosis versus Hartmann's procedures
Abstract
Objective: To compare primary resection and anastomosis (PRA) with and without defunctioning stoma to Hartmann's procedure (HP) as the optimal operative strategy for patients presenting with Hinchey stage III-IV, perforated diverticulitis.
Summary background data: The choice of operation for perforated diverticulitis lies between HP and PRA. Postoperative mortality and morbidity can be high, and the long-term consequences life-altering, with no established criteria guiding clinicians towards selecting a particular procedure.
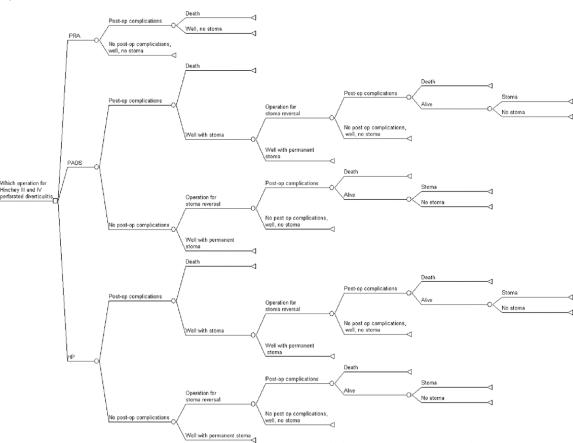
Methods: Probability estimates for 6879 patients with Hinchey III-IV perforated diverticulitis were obtained from two databases (n = 204), supplemented by expert opinion and summary data from 12 studies (n = 6675) published between 1980 and 2005. The primary outcome was quality-adjusted life-years (QALYs) gained from each strategy. Factors considered were the risk of permanent stoma, morbidity, and mortality from the primary or reversal operations. Decision analysis from the patient's perspective was used to calculate the optimal operative strategy and sensitivity analysis performed.
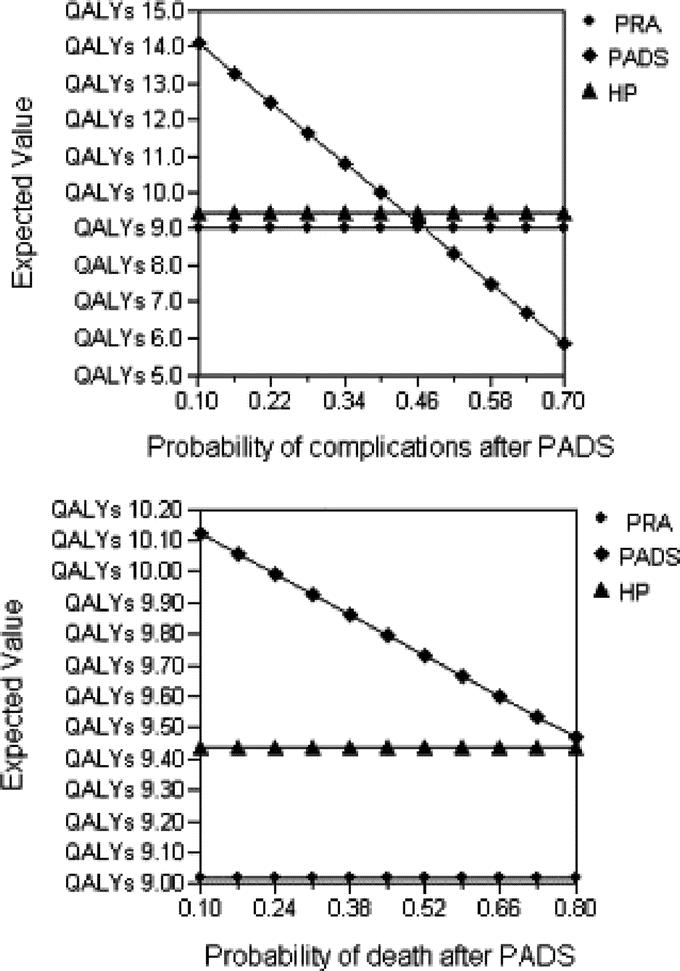
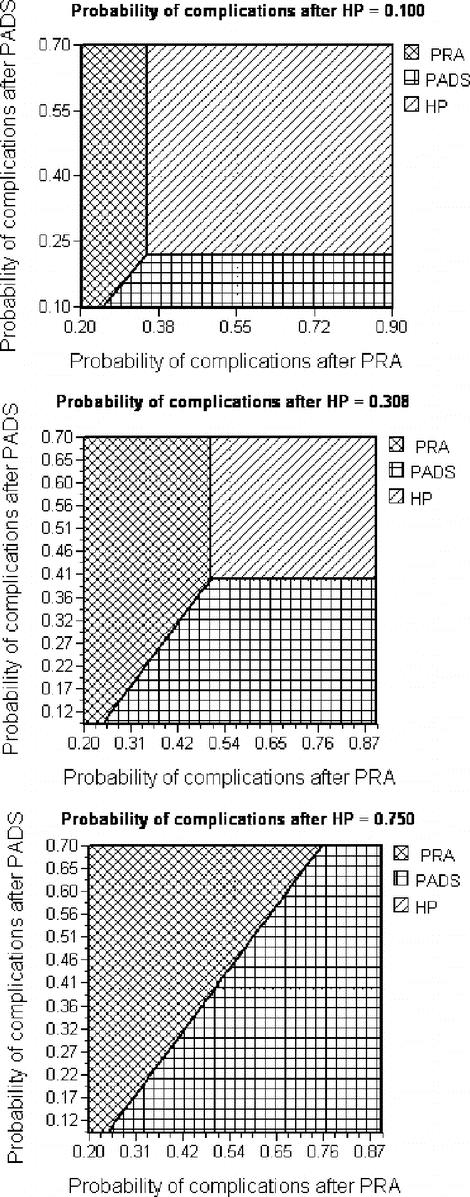
Results: A total of 135 PRA, 126 primary anastomoses with defunctioning stoma (PADS), and 6619 Hartmann's procedures (HP) were considered. The probability of morbidity and mortality was 55% and 30% for PRA, 40% and 25% for PADS, and 35% and 20% for HP, respectively. Stomas remained permanent in 27% of HP and in 8% of PADS. Analysis revealed the optimal strategy to be PADS with 9.98 QALYs, compared with 9.44 QALYs after HP and 9.02 QALYs after PRA. Complications after PRA reduced patients QALYs to a baseline of 2.713. Patients with postoperative complications during both primary and reversal operations for PADS and HP had QALYs of 0.366 and 0.325, respectively. HP became the optimal strategy only when risk of complications after PRA and PADS reached 50% and 44%, respectively.
Conclusion: Primary anastomosis with defunctioning stoma may be the optimal strategy for selected patients with diverticular peritonitis as may represent a good compromise between postoperative adverse events, long-term quality of life and risk of permanent stoma. HP may be reserved for patients with risk of complications >40% to 50% after consideration of long-term implications.
Figures
References
-
- Wong WD, Wexner SD, Lowry A, et al. Practice parameters for the treatment of sigmoid diverticulitis-supporting documentation: the Standards Task Force. The American Society of Colon and Rectal Surgeons. Dis Colon Rectum. 2000;43:290–297. - PubMed
-
- Makela J, Kiviniemi H, Laitinen S. Prevalence of perforated sigmoid diverticulitis is increasing. Dis Colon Rectum. 2002;45:955–961. - PubMed
-
- Zeitoun G, Laurent A, Rouffet F, et al. Multicentre, randomized clinical trial of primary versus secondary sigmoid resection in generalized peritonitis complicating sigmoid diverticulitis. Br J Surg. 2000;87:1366–1374. - PubMed
-
- Kronborg O. Treatment of perforated sigmoid diverticulitis: a prospective randomized trial. Br J Surg. 1993;80:505–507. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
