

The structure and function of the Rh antigen complex
- PMID: 17198846
- PMCID: PMC1831834
- DOI: 10.1053/j.seminhematol.2006.09.010
The structure and function of the Rh antigen complex
Abstract
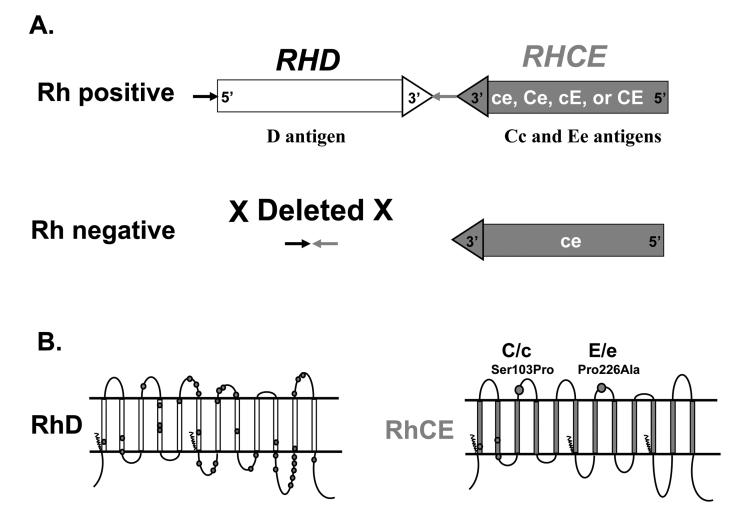
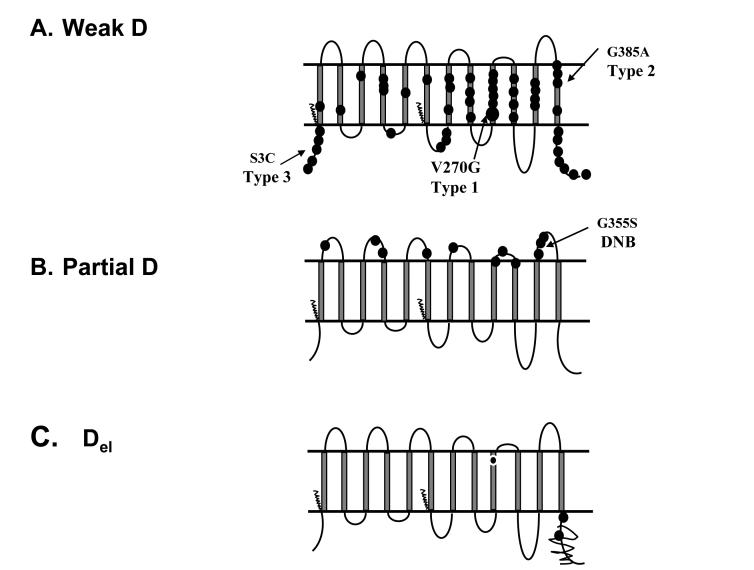
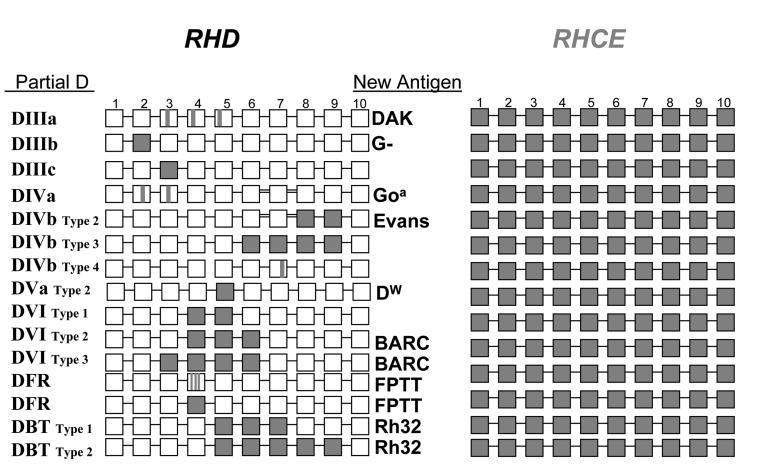
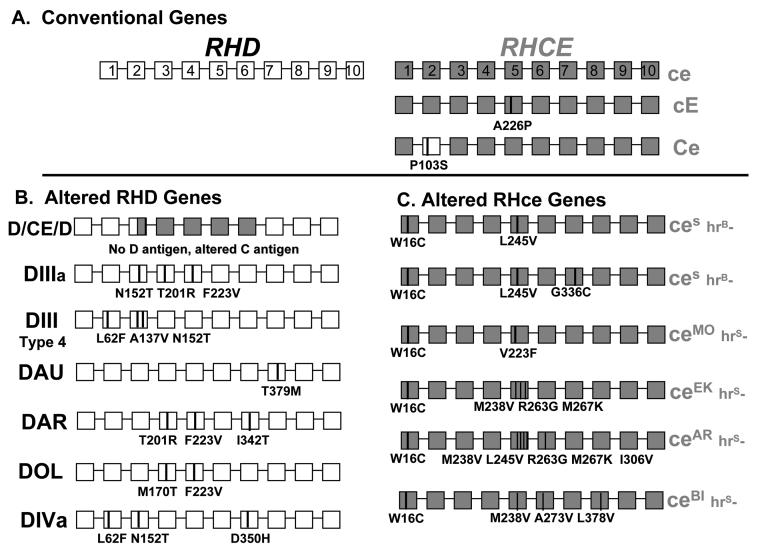
The Rh system is one of the most important and complex blood group systems because of the large number of antigens and the serious complications for the fetus of a woman sensitized by transfusion or pregnancy. Major advances in our understanding of the Rh system have occurred with the cloning of the genes and with functional evidence that the Rh blood group proteins belong to an ancient family of membrane proteins involved in ammonia transport. The arrangement and configuration of the genes at the RH locus promotes genetic exchange, generating new antigens. Importantly, RH genetic testing can now be applied to clinical transfusion medicine and prenatal practice. This includes testing for RHD zygosity, confirmation or resolution of D antigen status, and detection of altered RHD and RHCE genes in individuals at risk for producing antibodies to high-incidence Rh antigens, particularly sickle cell disease (SCD) patients. The Rh proteins form a core complex that is critical to the structure of the erythrocyte membrane, and they may play a physiologic role in the sequestration of blood ammonia. The Rh family of proteins now includes non-erythroid homologs present in many other tissues, and comparative genomics reveal Rh homologs in all domains of life.
Figures
References
-
- Levine P, Burnham L, Katzin WM, Vogel P. The role of isoimmunization in the pathogenesis of erythroblastosis fetalis. Am J Obstet Gynecol. 1941;42:925–937.
-
- Mollison PL, Hughes-Jones NC, Lindsay M, Wessely J. Suppression of primary RH immunization by passively-administered antibody. Experiments in volunteers. Vox Sang. 1969;16:421–439. - PubMed
-
- Freda V, Gorman J, Pollack W. Rh factor: Prevention of isoimmunization and clinical trials in mothers. Science. 1966;151:828–830. - PubMed
-
- Ballas S, Clark MR, Mohandas N, et al. Red cell membranes and cation deficiency in Rhnull syndrome. Blood. 1984;63:1046–1055. - PubMed
-
- Bruce LJ, Ghosh S, King MJ, et al. Absence of CD47 in protein 4.2-deficient hereditary spherocytosis in man: an interaction between the Rh complex and the band 3 complex. Blood. 2002;100:1878–1885. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
