

H pylori infection and systemic antibodies to CagA and heat shock protein 60 in patients with coronary heart disease
- PMID: 17203526
- PMCID: PMC4087548
- DOI: 10.3748/wjg.v12.i48.7815
H pylori infection and systemic antibodies to CagA and heat shock protein 60 in patients with coronary heart disease
Abstract
Aim: to determine the overall prevalence of H pylori and CagA positive H pylori infection and the prevalence of other bacterial and viral causes of chronic infection in patients with coronary heart disease (CHD), and the potential role of anti-heat-shock protein 60 (Hsp60) antibody response to these proteins in increasing the risk of CHD development.
Methods: Eighty patients with CHD and 160 controls were employed. We also compared the levels of anti-heat-shock protein 60 (Hsp60) antibodies in the two groups. The H pylori infection and the CagA status were determined serologically, using commercially available enzyme-linked immunosorbent assays (ELISA), and a Western blotting method developed in our laboratory. Systemic antibodies to Hsp60 were determined by a sandwich ELISA, using a polyclonal antibody to Hsp60 to sensitise polystyrene plates and a commercially available human Hsp60 as an antigen.
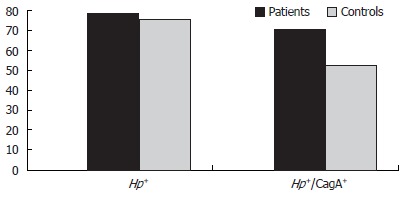
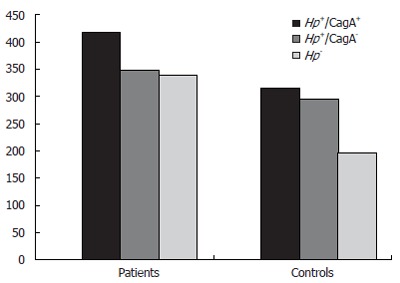
Results: The overall prevalence of H pylori infection was 78.7% (n = 63) in patients and 76.2% (n = 122) in controls (P = 0.07). Patients infected by CagA-positive (CagA+) H pylori strains were 71.4% (n = 45) vs 52.4% of infected controls (P = 0.030, OR = 2.27). Systemic levels of IgG to Hsp60 were increased in H pylori-negative patients compared with uninfected controls (P < 0.001) and CagA-positive infected patients compared with CagA-positive infected controls (P = 0.007).
Conclusion: CagA positive H pylori infection may concur to the development of CHD; high levels of anti-Hsp60 antibodies may constitute a marker and/or a concomitant pathogenic factor of the disease.
Figures
Similar articles
-
Serum levels of high-sensitivity C-reactive protein (hs-CRP)in Helicobacter pylori-infected peptic ulcer patients and its association with bacterial CagA virulence factor.Dig Dis Sci. 2009 Dec;54(12):2612-6. doi: 10.1007/s10620-008-0686-z. Dig Dis Sci. 2009. PMID: 19160050
-
Comparative study on antibodies to human and bacterial 60 kDa heat shock proteins in a large cohort of patients with coronary heart disease and healthy subjects.Eur J Clin Invest. 2001 Apr;31(4):285-92. doi: 10.1046/j.1365-2362.2001.00819.x. Eur J Clin Invest. 2001. PMID: 11298774
-
The infection by Helicobacter pylori strains expressing CagA is highly prevalent in women with autoimmune thyroid disorders.J Physiol Pharmacol. 1999 Dec;50(5):817-26. J Physiol Pharmacol. 1999. PMID: 10695561
-
Systematic review with meta-analysis: association between Helicobacter pylori CagA seropositivity and odds of inflammatory bowel disease.Aliment Pharmacol Ther. 2019 Jul;50(2):121-131. doi: 10.1111/apt.15306. Epub 2019 Jun 5. Aliment Pharmacol Ther. 2019. PMID: 31165513 Free PMC article.
-
Chronic infections and atherosclerosis.Ann N Y Acad Sci. 2007 Jun;1108:594-602. doi: 10.1196/annals.1422.062. Ann N Y Acad Sci. 2007. PMID: 17894024 Review.
Cited by
-
Impact of Helicobacter pylori Infection and Outcome of Anti-Helicobacter pylori Therapy in Patients with Reflux Laryngopharyngitis.Evid Based Complement Alternat Med. 2022 Jul 5;2022:8266321. doi: 10.1155/2022/8266321. eCollection 2022. Evid Based Complement Alternat Med. 2022. PMID: 35836834 Free PMC article.
-
Helicobacter Pylori-Induced Gastric Infections: From Pathogenesis to Novel Therapeutic Approaches Using Silver Nanoparticles.Pharmaceutics. 2022 Jul 14;14(7):1463. doi: 10.3390/pharmaceutics14071463. Pharmaceutics. 2022. PMID: 35890358 Free PMC article. Review.
-
Serum levels of high-sensitivity C-reactive protein (hs-CRP)in Helicobacter pylori-infected peptic ulcer patients and its association with bacterial CagA virulence factor.Dig Dis Sci. 2009 Dec;54(12):2612-6. doi: 10.1007/s10620-008-0686-z. Dig Dis Sci. 2009. PMID: 19160050
-
Advantages of Moxifloxacin and Levofloxacin-based triple therapy for second-line treatments of persistent Helicobacter pylori infection: a meta analysis.Wien Klin Wochenschr. 2010 Jul;122(13-14):413-22. doi: 10.1007/s00508-010-1404-3. Epub 2010 Jul 16. Wien Klin Wochenschr. 2010. PMID: 20628905
-
Clinical significance of Helicobacter pylori infection in patients with acute coronary syndromes: an overview of current evidence.Clin Res Cardiol. 2014 Nov;103(11):855-86. doi: 10.1007/s00392-014-0720-4. Epub 2014 May 10. Clin Res Cardiol. 2014. PMID: 24817551 Review.
References
-
- Pasceri V, Cammarota G, Patti G, Cuoco L, Gasbarrini A, Grillo RL, Fedeli G, Gasbarrini G, Maseri A. Association of virulent Helicobacter pylori strains with ischemic heart disease. Circulation. 1998;97:1675–1679. - PubMed
-
- Epstein SE, Zhou YF, Zhu J. Infection and atherosclerosis: emerging mechanistic paradigms. Circulation. 1999;100:e20–e28. - PubMed
-
- Epstein SE. The multiple mechanisms by which infection may contribute to atherosclerosis development and course. Circ Res. 2002;90:2–4. - PubMed
-
- Graham DY. Campylobacter pylori and peptic ulcer disease. Gastroenterology. 1989;96:615–625. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
