

The waiting time for inter-country spread of pandemic influenza
- PMID: 17206278
- PMCID: PMC1764036
- DOI: 10.1371/journal.pone.0000143
The waiting time for inter-country spread of pandemic influenza
Abstract
Background: The time delay between the start of an influenza pandemic and its subsequent initiation in other countries is highly relevant to preparedness planning. We quantify the distribution of this random time in terms of the separate components of this delay, and assess how the delay may be extended by non-pharmaceutical interventions.
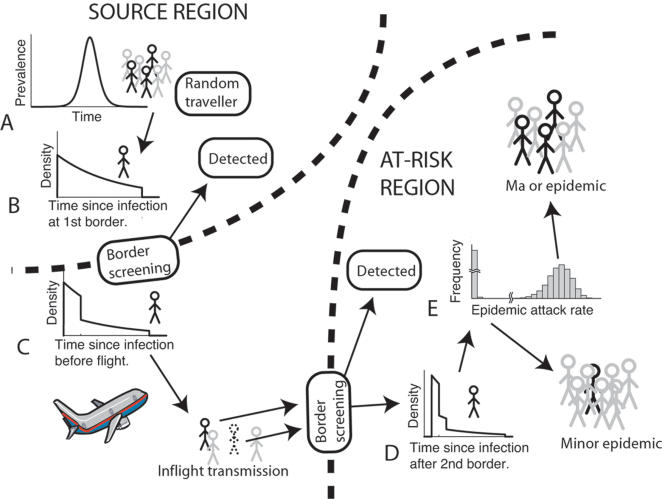
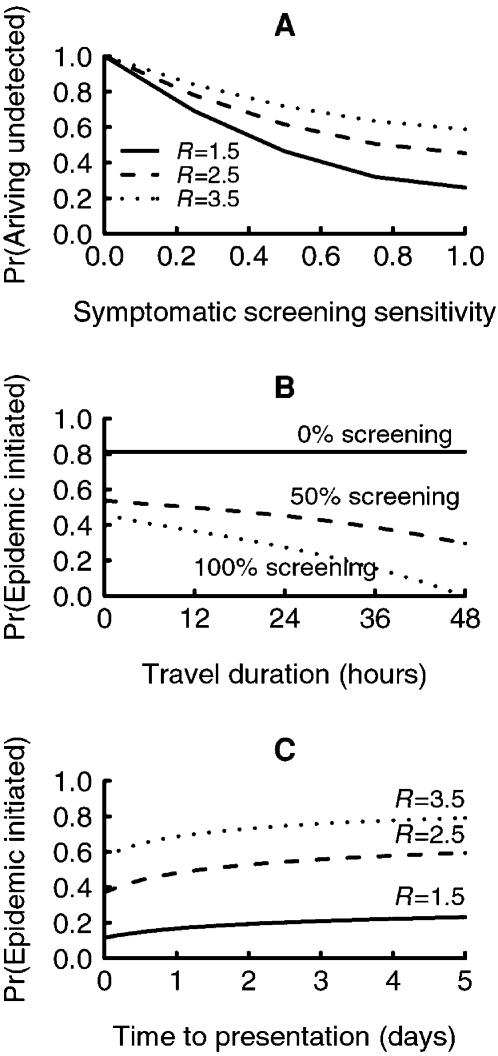
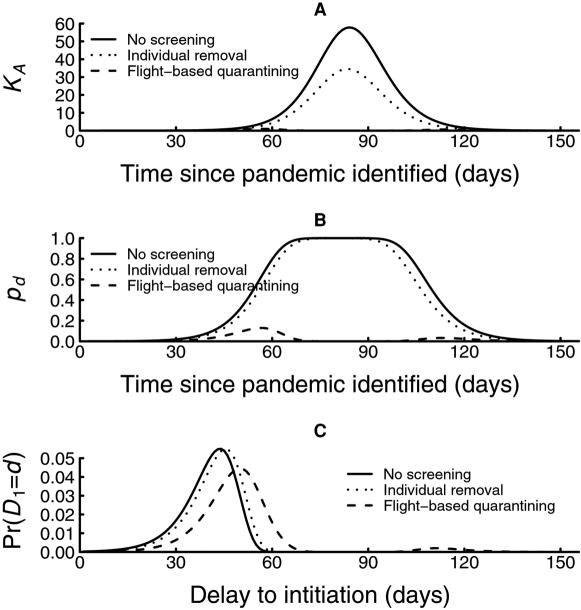
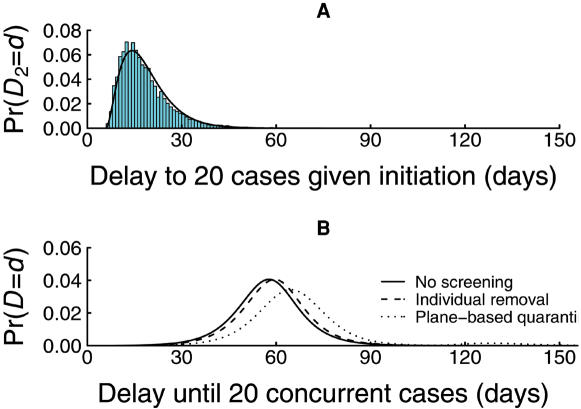
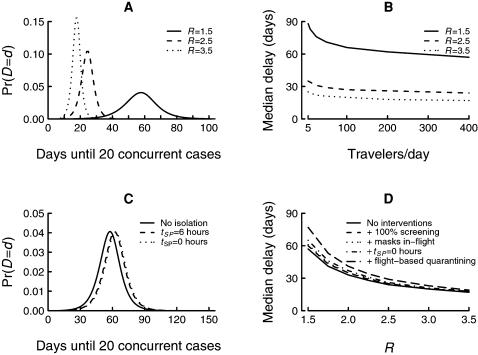
Methods and findings: The model constructed for this time delay accounts for: (i) epidemic growth in the source region, (ii) the delay until an infected individual from the source region seeks to travel to an at-risk country, (iii) the chance that infected travelers are detected by screening at exit and entry borders, (iv) the possibility of in-flight transmission, (v) the chance that an infected arrival might not initiate an epidemic, and (vi) the delay until infection in the at-risk country gathers momentum. Efforts that reduce the disease reproduction number in the source region below two and severe travel restrictions are most effective for delaying a local epidemic, and under favourable circumstances, could add several months to the delay. On the other hand, the model predicts that border screening for symptomatic infection, wearing a protective mask during travel, promoting early presentation of cases arising among arriving passengers and moderate reduction in travel volumes increase the delay only by a matter of days or weeks. Elevated in-flight transmission reduces the delay only minimally.
Conclusions: The delay until an epidemic of pandemic strain influenza is imported into an at-risk country is largely determined by the course of the epidemic in the source region and the number of travelers attempting to enter the at-risk country, and is little affected by non-pharmaceutical interventions targeting these travelers. Short of preventing international travel altogether, eradicating a nascent pandemic in the source region appears to be the only reliable method of preventing country-to-country spread of a pandemic strain of influenza.
Conflict of interest statement
Figures
References
-
- Ferguson NM, Cummings DAT, Cauchemez S, Fraser C, Riley S, et al. Strategies for containing an emerging influenza pandemic in Southeast Asia. Nature. 2005;437:209214. - PubMed
-
- Longini IM, Nizam A, Xu S, Ungchusak K, Hanshoaworakul W, et al. Containing pandemic influenza at the source. Science. 2005;309:1083–1087. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
