

Antiviral therapy and resistance with hepatitis B virus infection
- PMID: 17206760
- PMCID: PMC4065869
- DOI: 10.3748/wjg.v13.i1.125
Antiviral therapy and resistance with hepatitis B virus infection
Abstract
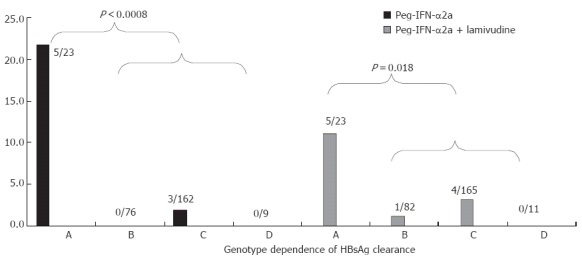
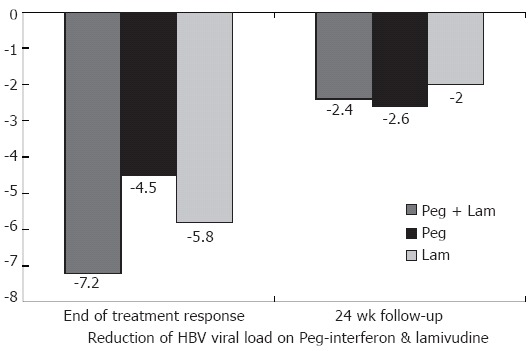
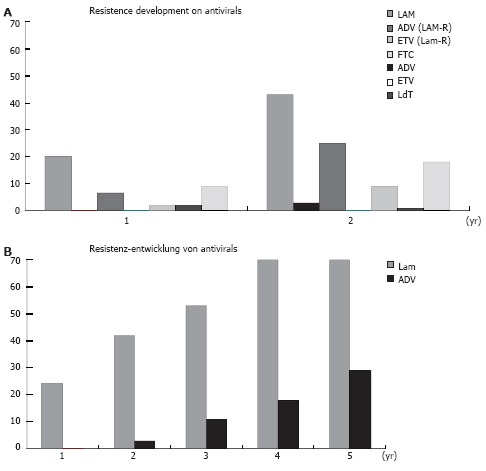
Hepatitis B virus (HBV) infection is still the most common cause of hepatocellular carcinoma and liver cirrhosis world wide. Recently, however, there has been quite dramatic improvement in the understanding of HBV associated liver disease and its treatment. It has become clear that high viral replication is a major risk factor for the development of both cirrhosis and hepatocellular carcinoma. Early studies have shown lamivudine lowers the risk of HBV associated complications. There are currently three nucleos(t)ides licensed, in addition to interferon, and there are more drugs coming to the market soon. Interferon or its pegylated counterpart are still the only options for treatment with defined end points, while nucleos(t)ides therapy is used mostly for long term treatment. Combination therapies have not been shown to be superior to monotherapy in naive patients, however, the outcome depends on how the end point is defined. Interferon plus lamivudine achieves a higher viral suppression than either treatment alone, even though Hbe-seroconversion was not different after a one year treatment. HBV-genotypes emerge as relevant factors, with genotypes "A" and "B" responding relatively well to interferon, achieving up to 20% HBsAg clearance in the case of genotype "A". In addition to having a defined treatment duration, interferon has the advantage of lacking resistance selection, which is a major drawback for lamivudine and the other nucleos(t)ides. The emergence of resistance against adefovir and entecavir is somewhat slower in naive compared to lamivudine resistant patients. Adefovir has a low resistance profile with 3%, 9%, 18%, and 28% after 2, 3, 4, and 5 years, respectively, while entecavir has rarely produced resistance in naive patients for up to 3 years.
Figures
References
-
- World Health Organization.Available from: http://www.who.int/csr/disease/hepatitis/HepatitisB_whocdscsrlyo2002_2.pdf.
-
- Chen CJ, Yang HI, Su J, Jen CL, You SL, Lu SN, Huang GT, Iloeje UH. Risk of hepatocellular carcinoma across a biological gradient of serum hepatitis B virus DNA level. JAMA. 2006;295:65–73. - PubMed
-
- Weller IV, Carreno V, Fowler MJ, Monjardino J, Makinen D, Thomas HC, Sherlock S. Acyclovir inhibits hepatitis B virus replication in man. Lancet. 1982;1:273. - PubMed
-
- Schalm SW. Treatment of chronic hepatitis type virus B. Hepatogastroenterology. 1984;31:12–16. - PubMed
-
- Sherlock S, Thomas HC. Treatment of chronic hepatitis due to hepatitis B virus. Lancet. 1985;2:1343–1346. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
