

Review
doi: 10.1102/1470-7330.2006.0032.
Upper gastrointestinal tumours: diagnosis and staging
Affiliations
- PMID: 17208679
- PMCID: PMC1766562
- DOI: 10.1102/1470-7330.2006.0032
Item in Clipboard
Review
Upper gastrointestinal tumours: diagnosis and staging
Cancer Imaging.
.
Abstract
Upper GI tumours have a dismal prognosis. Only early diagnosis and accurate staging can optimize patient management.
(c) International Cancer Imaging Society.
Figures
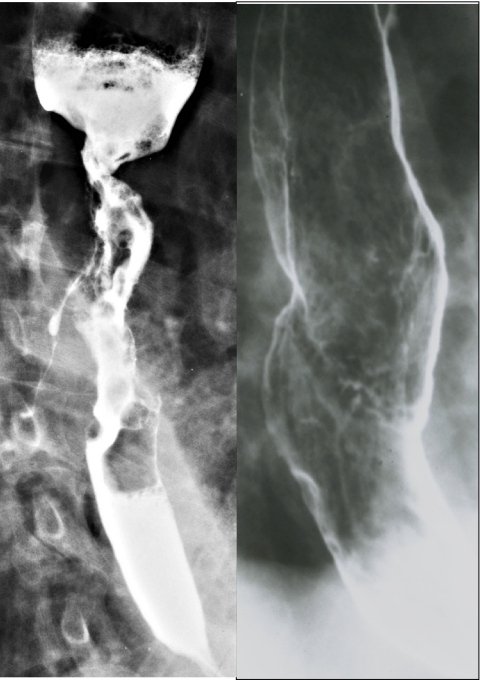
Carcinoma of the oesophagus on double contrast barium studies. (a) Squamous cell carcinoma showing luminal narrowing, abrupt shelf-like borders, ulceration, circumferential growth and a fistula to the tracheobronchial tree. (b) Adenocarcinoma arising from Barrett’s mucosa causes a benign-appearing stricture associated with a plaque-like tumour of the mid-oesophagus.
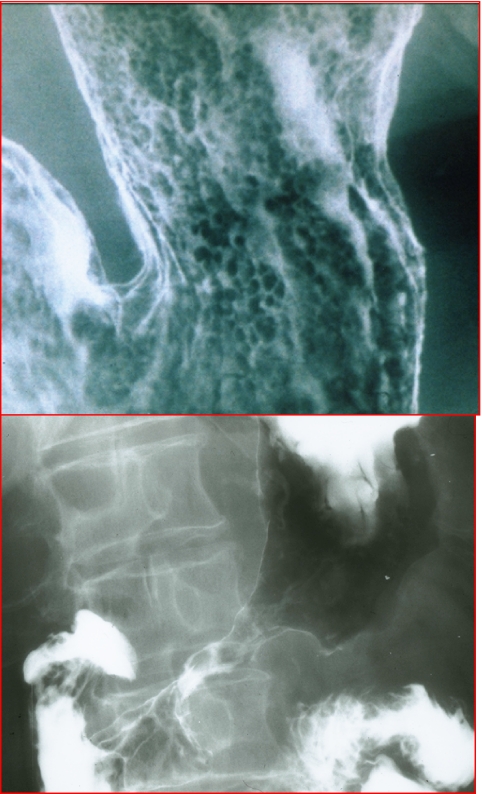
Adenocarcinoma of the stomach. (a) Early gastric cancer with mucosal nodularity. (b) Advanced gastric cancer with narrowing and rigidity of the antral wall due to mural infiltration of scabrous tumour.
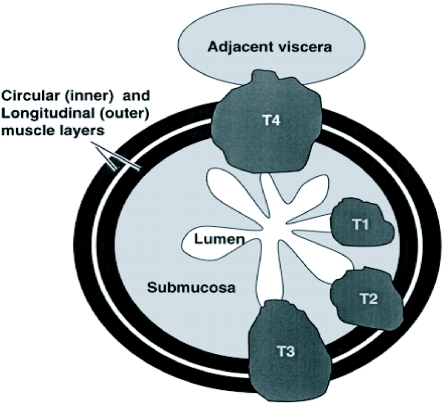
Schematic showing T staging of oesophageal and gastric cancer. T1, tumour extends into submucosa; T2, tumour extends into muscularis propria; T3, tumour extends through the muscularis propria into the subserosa; T4, tumour extends directly into other organs or tissues.
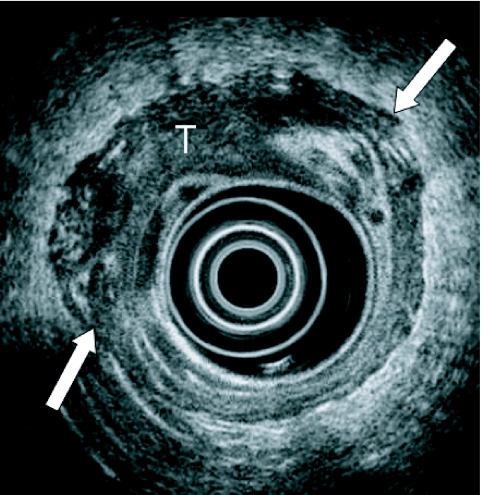
Endoscopic ultrasound demonstrates a T3 oesophageal neoplasm (T) that has invaded beyond the muscularis propria (arrows).
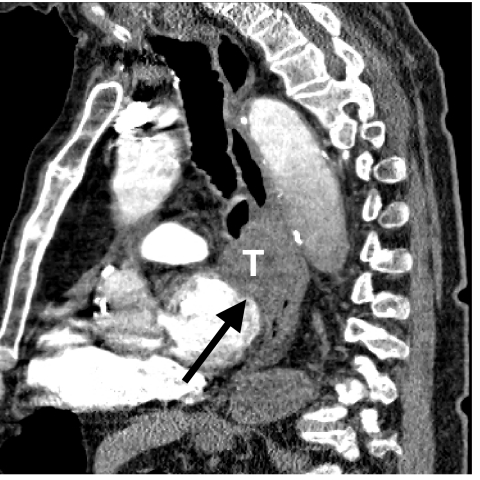
Sagittal reformatted image discloses a T4 tumour (T) invading the mediastinum and left atrial wall (arrow).
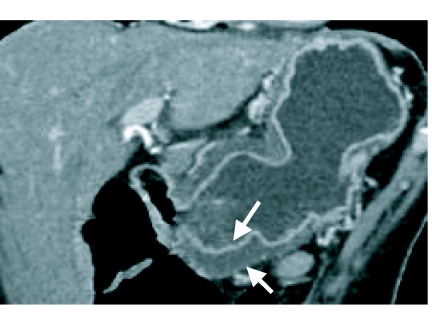
Coronal reformatted image of the stomach discloses a T2 tumour that is causing mural thickening of the gastric antrum (arrows) but no penetration beyond the muscularis propria.
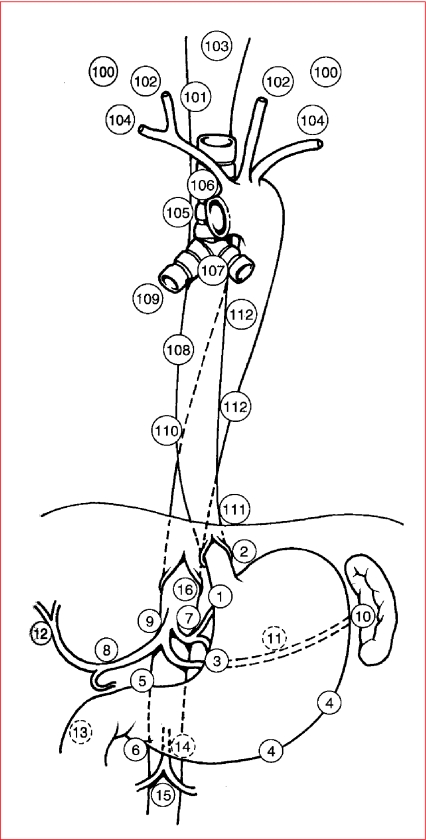
N staging of oesophago-gastric neoplasm. Schematic diagram depicting the common sites of lymph node metastases in oesophageal and gastric cancers.

Coronal reformatted image shows direct invasion (arrows) of a gastric cancer into the spleen via the gastrosplenic ligament.

Coronal reformatted image shows large Krukenberg tumours of the ovaries (arrows) due to hematogenous metastases from a gastric cancer (T).
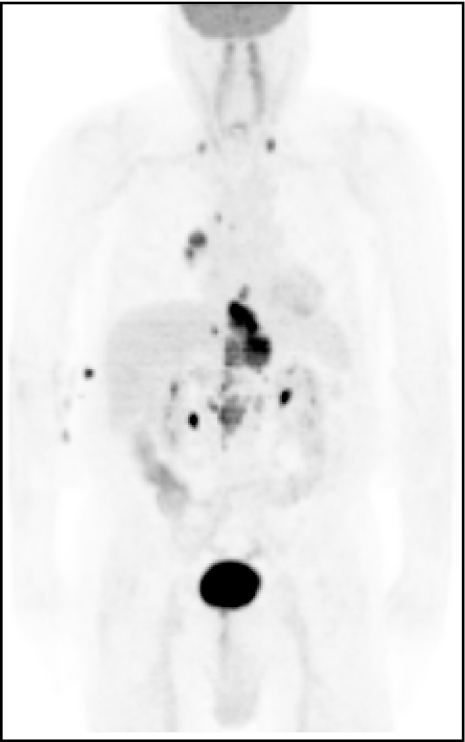
PET scan showing a tumour of the oesophago-gastric junction with metastatic disease to the chest and neck.
References
-
- Gore RM, Yaghmai V. Esophageal cancer. In: Bragg DG, Rubin P, Hricak H, editors. Oncologic Imaging. 2nd ed. Philadelphia: Saunders; 2002. pp. 359–90.
-
- Gore RM, Miller FH. Stomach cancer. In: Bragg DG, Rubin P, Hricak H, editors. Oncologic Imaging. 2nd ed. Philadelphia: Saunders; 2002. pp. 391–418.
-
- Lee SS, Ha HK, Shin YM, et al. Superficial esophageal cancer: esophagogastric findings correlated with histopathologic findings. Radiology. 2005;236:535–44. - PubMed
-
- Iyer RB, Silverman PM, Tamm EP, et al. Diagnosis, staging, and follow-up of esophageal cancer. AJR. 2003;181:785–93. - PubMed
-
- Iyer R, Dubrow R. Imaging upper gastrointestinal malignancy. Semin Roentgenol. 2006;41:113–20. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical