

Determinants of normal retinal nerve fiber layer thickness measured by Stratus OCT
- PMID: 17210181
- PMCID: PMC2916163
- DOI: 10.1016/j.ophtha.2006.08.046
Determinants of normal retinal nerve fiber layer thickness measured by Stratus OCT
Erratum in
- Ophthalmology. 2008 Mar;115(3):472
Abstract
Purpose: To determine the effects of age, optic disc area, ethnicity, eye, gender, and axial length on the retinal nerve fiber layer (RNFL) in the normal human eye as measured by Stratus OCT (optical coherence tomography).
Design: Cross-sectional observational study.
Participants: Three hundred twenty-eight normal subjects 18 to 85 years old.
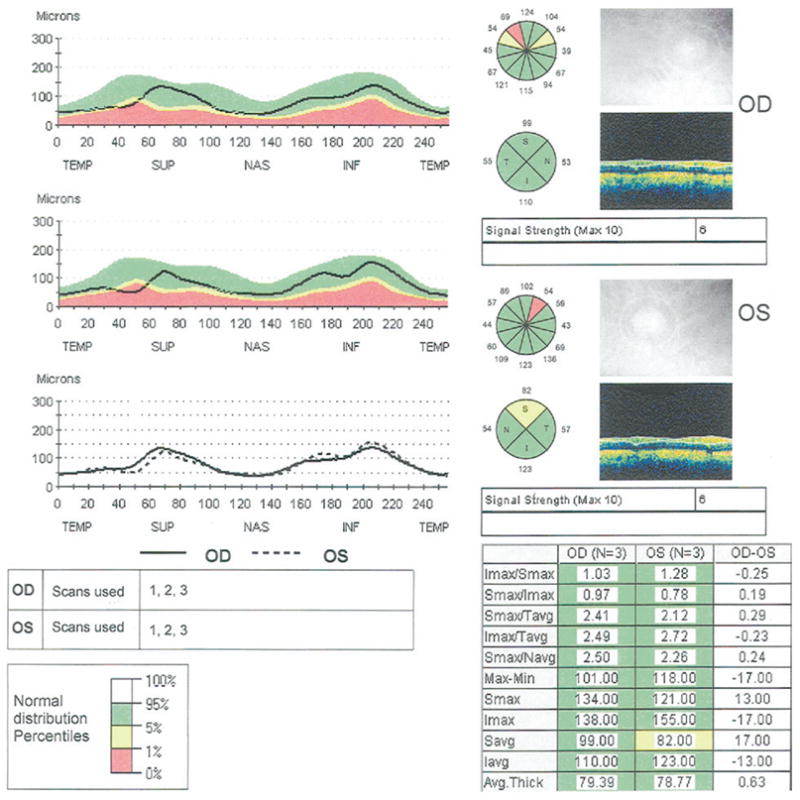
Methods: Peripapillary Fast RNFL scans performed by Stratus OCT with a nominal diameter of 3.46 mm centered on the optic disc were performed on one randomly selected eye of each subject.
Main outcome measures: Linear regression analysis of the effects of age, ethnicity, gender, eye, axial length, and optic disc area on peripapillary RNFL thickness.
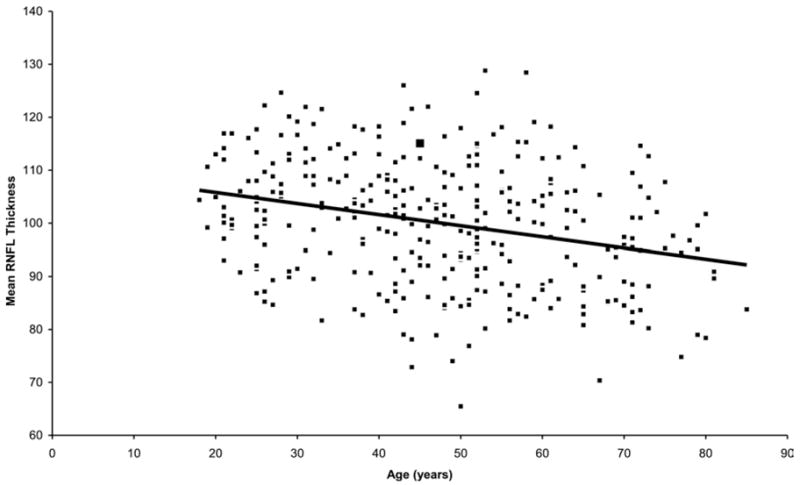
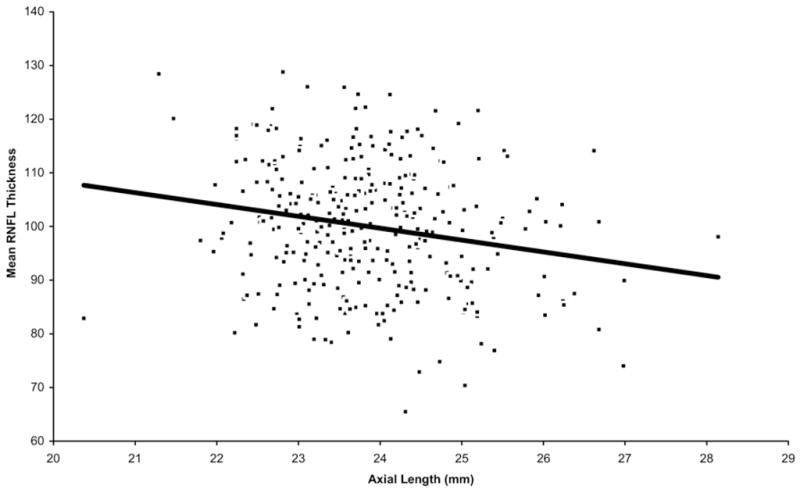
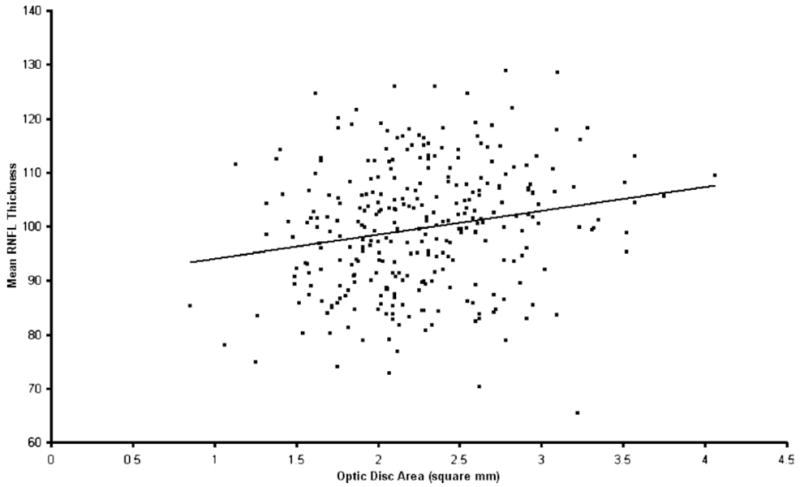
Results: The mean RNFL thickness for the entire population was 100.1 microm (standard deviation, 11.6). Thinner RNFL measurements were associated with older age (P<0.001); being Caucasian, versus being either Hispanic or Asian (P = 0.006); greater axial length (P<0.001); or smaller optic disc area (P = 0.010). For every decade of increased age, mean RNFL thickness measured thinner by approximately 2.0 microm (95% confidence interval [CI], 1.2-2.8). For every 1-mm-greater axial length, mean RNFL thickness measured thinner by approximately 2.2 microm (95% CI, 1.1-3.4). For every increase in square millimeter of optic disc area, mean RNFL thickness increased by approximately 3.3 microm (95% CI, 0.6-5.6). Comparisons between ethnic groups revealed that Caucasians had mean RNFL values (98.1+/-10.9 microm) slightly thinner than those of Hispanics (103.7+/-11.6 microm; P = 0.022) or Asians (105.8+/-9.2 microm; P = 0.043). There was no relationship between RNFL thickness and eye or gender.
Conclusions: Retinal nerve fiber layer thickness, as measured by Stratus OCT, varies significantly with age, ethnicity, axial length, and optic disc area. These variables may need to be taken into account when evaluating patients for diagnosis and follow-up of glaucoma, particularly at the lower boundary of the normal range. Due to the relatively small numbers of subjects of Asian and African descent in the normative database, conclusions regarding the effect of ethnicity should be interpreted with caution.
Figures
References
-
- American Academy of Ophthalmology Glaucoma Panel. Primary open-angle glaucoma. San Francisco: American Academy of Ophthalmology; 2003. [Accessed October 18, 2006]. Preferred Practice Pattern; p. 3. Available at: http://www.aao.org/education/library/ppp/upload/Primary_Open-Angle_Glauc....
-
- Kass MA, Heuer DK, Higginbotham EJ, et al. The Ocular Hypertension Treatment Study: a randomized trial determines that topical ocular hypotensive medication delays or prevents the onset of primary open-angle glaucoma. Arch Ophthalmol. 2002;120:701–13. - PubMed
-
- Quigley HA, Dunkelberger GR, Green WR. Retinal ganglion cell atrophy correlated with automated perimetry in human eyes with glaucoma. Am J Ophthalmol. 1989;107:453–64. - PubMed
-
- Mikelberg FS, Yidegiligne HM, Shulzer M. Optic nerve axon count and axon diameter in patients with ocular hypertension and normal visual fields. Ophthalmology. 1995;102:342–8. - PubMed
-
- Kerrigan-Baumrind LA, Quigley HA, Pease ME, et al. Number of ganglion cells in glaucoma eyes compared with threshold visual field tests in the same persons. Invest Ophthalmol Vis Sci. 2000;41:741–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
