

Treatment related morbidity of unruptured intracranial aneurysms: results of a prospective single centre series with an interdisciplinary approach over a 6 year period (1999-2005)
- PMID: 17210624
- PMCID: PMC2117727
- DOI: 10.1136/jnnp.2006.106823
Treatment related morbidity of unruptured intracranial aneurysms: results of a prospective single centre series with an interdisciplinary approach over a 6 year period (1999-2005)
Abstract
Objectives: To review the angiographic and clinical outcome of patients with unruptured intracranial aneurysm(s) (UIA) with regard to complications and successful obliteration by surgical clipping or endovascular coiling.
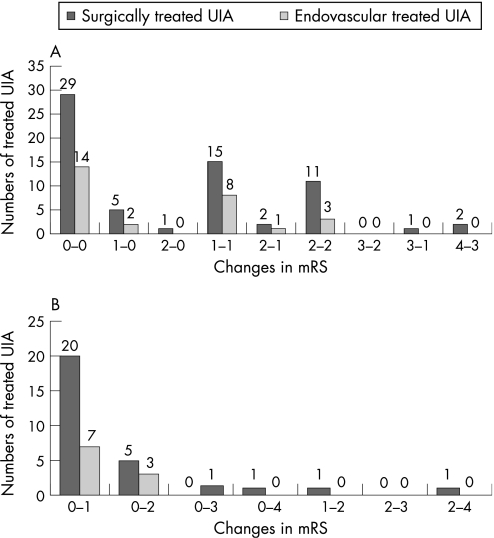
Methods: Data were derived from a prospective database of intracranial aneurysms from June 1999 to May 2005. All patients were followed-up for 6 months using the modified Rankin Scale (mRS). Favourable outcome was classified as mRS 0-2. From a total of 691 patients included in the database, 173 harboured 206 UIA of whom 118 patients (133 UIA) were treated.
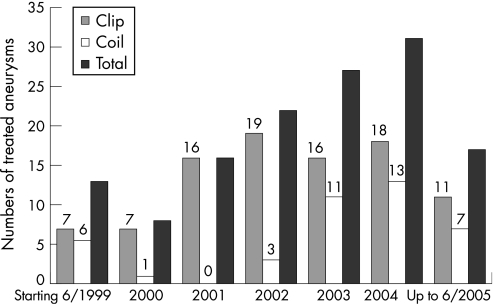
Results: Primary treatment assignment was surgical repair in 91 UIA and endovascular treatment in 42. In 3 UIA (7.1%), endovascular treatment was not feasible and had to be abandoned. Definite treatment was surgery in 94 UIA (81 patients) and endovascular obliteration in 39 UIA (37 patients). There were no deaths related to any treatment. Immediately after treatment, 6.4% of the surgical and 7.7% of the endovascular patients showed new neurological deficits, mainly related to cerebral ischaemia. After 6 months, 3 (2.3%) patients had a treatment related unfavourable outcome, defined as mRS >2, 2 patients after surgical and 1 patient after endovascular aneurysm repair (not statistically different, p = 0.3; Fisher's exact test). This led to an overall satisfactory outcome in 97.9% of surgically and 97.4% of endovasculary treated UIA. After surgical clipping, complete occlusion of the aneurysm was achieved in 88 (93.6%) and near complete (small residual neck) in 4 (4.3%) of 94 UIA. Two small posterior communicating artery aneurysms with a fetal type posterior communicating artery were wrapped. After endovascular treatment, obliteration was complete in 26 (66.7%). Small residual neck was seen in 13 (33.3%), but none of the UIA showed residual aneurysm filling. Five patients in the endovascular group (13.9%) underwent repeated endovascular treatment after aneurysm recanalisation.
Conclusions: If patients are carefully selected and individually assigned to their optimum treatment modality, UIA can be obliterated by surgery or endovascular treatment in the majority of patients, with a low percentage of unfavourable outcomes. In this series, the outcome was not dependent on treatment. However, the rate of recanalisation of UIA is higher after endovascular obliteration. After diagnosis of an UIA, an individual interdisciplinary decision is essential for each patient to provide the optimum management.
References
-
- Unruptured intracranial aneurysms—risk of rupture and risks of surgical intervention. International Study of Unruptured Intracranial Aneurysms Investigators. N Engl J Med 19983391725–1733. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical