

Attainment of clinical performance targets and improvement in clinical outcomes and resource use in hemodialysis care: a prospective cohort study
- PMID: 17212829
- PMCID: PMC1783649
- DOI: 10.1186/1472-6963-7-5
Attainment of clinical performance targets and improvement in clinical outcomes and resource use in hemodialysis care: a prospective cohort study
Abstract
Background: Clinical performance targets are intended to improve patient outcomes in chronic disease through quality improvement, but evidence of an association between multiple target attainment and patient outcomes in routine clinical practice is often lacking.
Methods: In a national prospective cohort study (ESRD Quality, or EQUAL), we examined whether attainment of multiple targets in 668 incident hemodialysis patients from 74 U.S. not-for-profit dialysis clinics was associated with better outcomes. We measured whether the following accepted clinical performance targets were met at 6 months after study enrollment: albumin (> or =4.0 g/dl), hemoglobin (> or =11 g/dl), calcium-phosphate product (<55 mg2/dl2), dialysis dose (Kt/V> or =1.2), and vascular access type (fistula). Outcomes included mortality, hospital admissions, hospital days, and hospital costs.
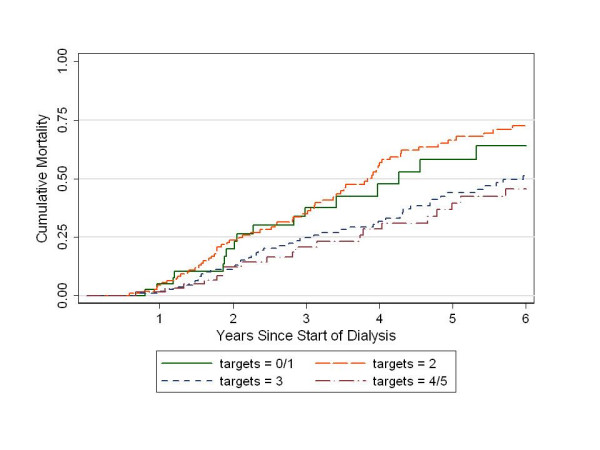
Results: Attainment of each of the five targets was associated individually with better outcomes; e.g., patients who attained the albumin target had decreased mortality [relative hazard (RH) = 0.55, 95% confidence interval (CI), 0.41-0.75], hospital admissions [incidence rate ratio (IRR) = 0.67, 95% CI, 0.62-0.73], hospital days (IRR = 0.61, 95% CI, 0.58-0.63), and hospital costs (average annual cost reduction = 3,282 dollars, P = 0.002), relative to those who did not. Increasing numbers of targets attained were also associated, in a graded fashion, with decreased mortality (P = 0.030), fewer hospital admissions and days (P < 0.001 for both), and lower costs (P = 0.029); these trends remained statistically significant for all outcomes after adjustment (P < 0.001), except cost, which was marginally significant (P = 0.052).
Conclusion: Attainment of more clinical performance targets, regardless of which targets, was strongly associated with decreased mortality, hospital admissions, and resource use in hemodialysis patients.
Figures
References
-
- Committee on Quality of Health Care in America IM, editor. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC, National Academy Press; 2001.
-
- Lacson E, Jr, Teng M, Lazarus JM, Lew N, Lowrie E, Owen W. Limitations of the facility-specific standardized mortality ratio for profiling health care quality in dialysis. Am J Kidney Dis. 2001;37:267–275. - PubMed
-
- Foundation NK. Kidney Disease Outcomes Quality Initiative (K/DOQI). http://www.kidney.org/professionals/doqi. 2005. http://www.kidney.org/professionals/KDOQI/
-
- Lowrie EG, Huang WH, Lew NL. Death risk predictors among peritoneal dialysis and hemodialysis patients: a preliminary comparison. Am J Kidney Dis. 1995;26:220–228. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
