

doi: 10.1186/1749-7922-2-1.
State of the art: noninvasive imaging and management of neurovascular trauma
Affiliations
- PMID: 17212833
- PMCID: PMC1796545
- DOI: 10.1186/1749-7922-2-1
Item in Clipboard
State of the art: noninvasive imaging and management of neurovascular trauma
World J Emerg Surg.
.
Abstract
Neurotrauma represents a significant public health problem, accounting for a significant proportion of the morbidity and mortality associated with all traumatic injuries. Both blunt and penetrating injuries to cervicocerebral vessels are significant and are likely more common than previously recognized. Imaging of such injuries is an important component in the evaluation of individuals presenting with such potential injuries, made all the more important since many of the vascular injuries are clinically silent. Management of injuries, particularly those caused by blunt trauma, is constantly evolving. This article addresses the current state of imaging and treatment of such injuries.
Figures

53-year old Korean man with a remote history of facial trauma, and a four day history of diplopia and right third cranial nerve palsy. Lateral digital subtraction angiogram, right internal carotid artery. During this early phase, there is visualization of the cervical and intracranial carotid artery; in addition, early filling of the cavernous sinus (arrow) is noted.
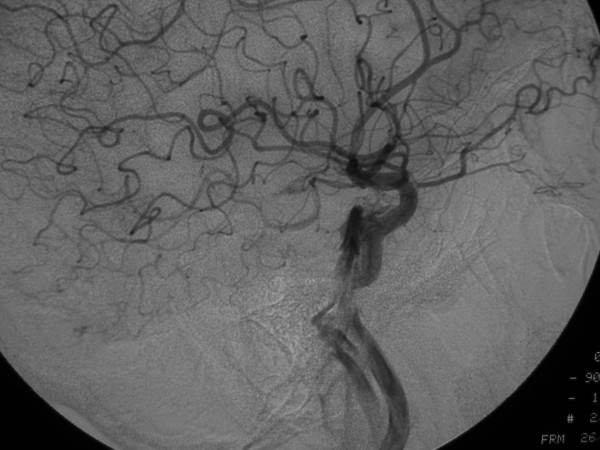
53-year old Korean man with a remote history of facial trauma, and a four day history of diplopia and right third cranial nerve palsy. Lateral digital subtraction angiogram, right internal carotid artery. Later image from the same angiogram as Figure 1A, demonstrating further filling of the cavernous sinus and draining veins.

53-year old Korean man with a remote history of facial trauma, and a four day history of diplopia and right third cranial nerve palsy. Anteroposterior digital subtraction angiogram, right internal carotid artery. Mid-arterial phase image demonstrates early filling of the cavernous sinus with filling of the contralateral inferior petrosal sinus (arrow).

Anomalous origin on the right subclavian artery. Serial images from a helical CT scan of the superior mediastinum, cranial to caudal. Notice the large enhancing vascular structure posterior to the esophagus (*). On the more caudal images, a direct origin of this vessel from the aortic arch, distal to the origin of the left subclavian artery, is noted.
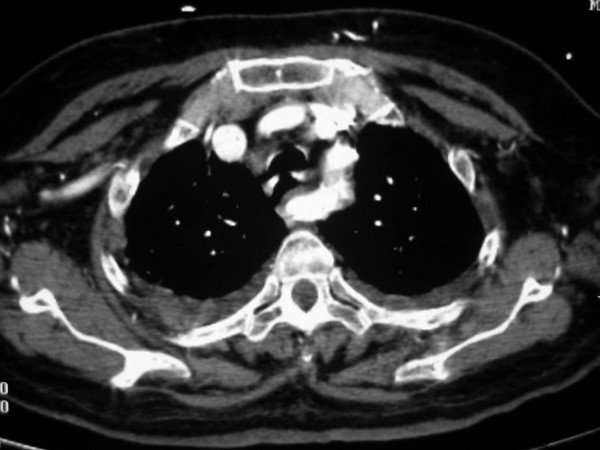
Anomalous origin on the right subclavian artery. Serial images from a helical CT scan of the superior mediastinum, cranial to caudal. Notice the large enhancing vascular structure posterior to the esophagus (*). On the more caudal images, a direct origin of this vessel from the aortic arch, distal to the origin of the left subclavian artery, is noted.

Anomalous origin on the right subclavian artery. Serial images from a helical CT scan of the superior mediastinum, cranial to caudal. Notice the large enhancing vascular structure posterior to the esophagus (*). On the more caudal images, a direct origin of this vessel from the aortic arch, distal to the origin of the left subclavian artery, is noted.

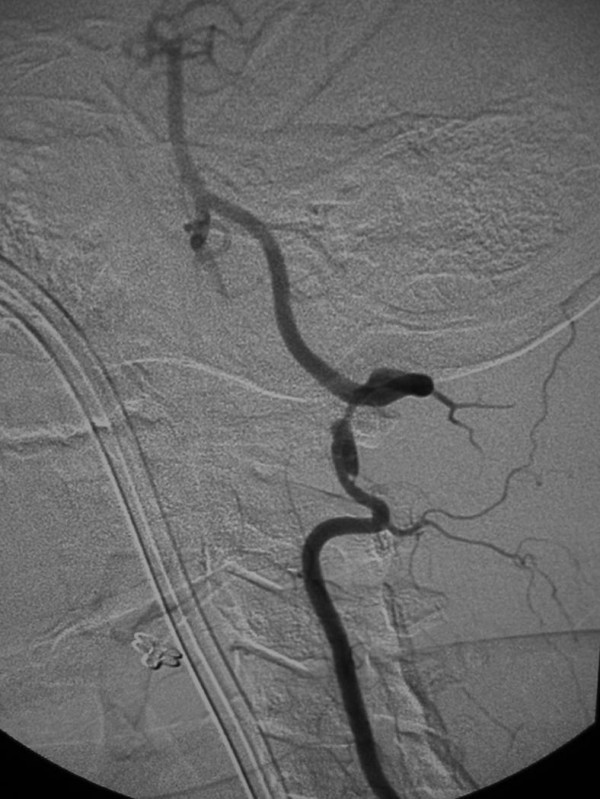
36-year old woman, s/p motor vehicle collision. On admission, an angiogram demonstrated a pseudoaneurysm of the thoracic aorta, as well as a grade 3 (pseudoaneurysm) of her left internal carotid artery. Her aorta was repaired immediately; on follow-up angiography of her carotid injury, her pseudoaneurysm had progressed and there was significant narrowing of the adjacent internal carotid artery. Digital subtraction angiogram of the left internal carotid artery, 7-days following initial injury. There is a pseudoaneurysm (arrow) of the proximal internal carotid artery with narrowing of the adjacent artery. A second, smaller pseudoaneurysm (arrowhead) is noted in the more distal artery.

36-year old woman, s/p motor vehicle collision. On admission, an angiogram demonstrated a pseudoaneurysm of the thoracic aorta, as well as a grade 3 (pseudoaneurysm) of her left internal carotid artery. Her aorta was repaired immediately; on follow-up angiography of her carotid injury, her pseudoaneurysm had progressed and there was significant narrowing of the adjacent internal carotid artery. Digital subtraction angiogram of the left internal carotid artery, s/p stent placement. A 6 mm × 47 mm Magic Wallstent (Boston Scientific, Watertown, MA) was placed. Notice the immediate and nearly complete resolution of the pseudoaneurysms.

36-year old woman, s/p motor vehicle collision. On admission, an angiogram demonstrated a pseudoaneurysm of the thoracic aorta, as well as a grade 3 (pseudoaneurysm) of her left internal carotid artery. Her aorta was repaired immediately; on follow-up angiography of her carotid injury, her pseudoaneurysm had progressed and there was significant narrowing of the adjacent internal carotid artery. Unsubtracted image demonstrating the cervical stent (arrows).
25-year old woman involved in a rollover motor vehicle collision. On admission to the hospital, a screening four-vessel angiogram revealed a pseudoaneurysm of the left vertebral artery at the level of the C1–C2 disc space. Follow-up angiography performed 7 days later revealed enlargement of the pseudoaneurysm and concomitant narrowing of the vertebral artery. Due to the tortuosity of the vertebral artery, stent placement was not deemed a viable option and the vertebral artery was embolized. Lateral digital subtraction angiogram, left vertebral artery. Notice the pseudoaneurysm arising from the distal vertebral artery (arrow), and the adjacent vertebral artery narrowing.
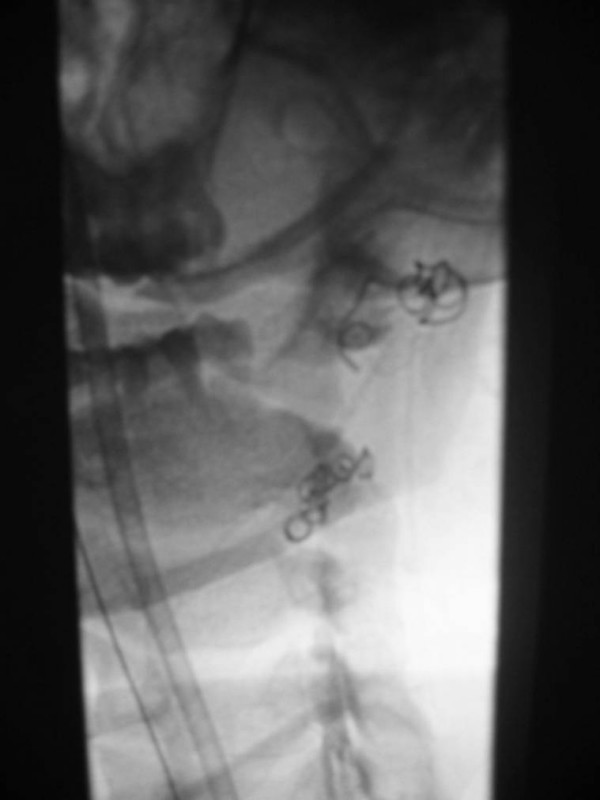
25-year old woman involved in a rollover motor vehicle collision. On admission to the hospital, a screening four-vessel angiogram revealed a pseudoaneurysm of the left vertebral artery at the level of the C1–C2 disc space. Follow-up angiography performed 7 days later revealed enlargement of the pseudoaneurysm and concomitant narrowing of the vertebral artery. Due to the tortuosity of the vertebral artery, stent placement was not deemed a viable option and the vertebral artery was embolized. Unsubtracted image demonstrating coils placed distal and proximal to the pseudoaneurysm, trapping the diseased segment of vessel.
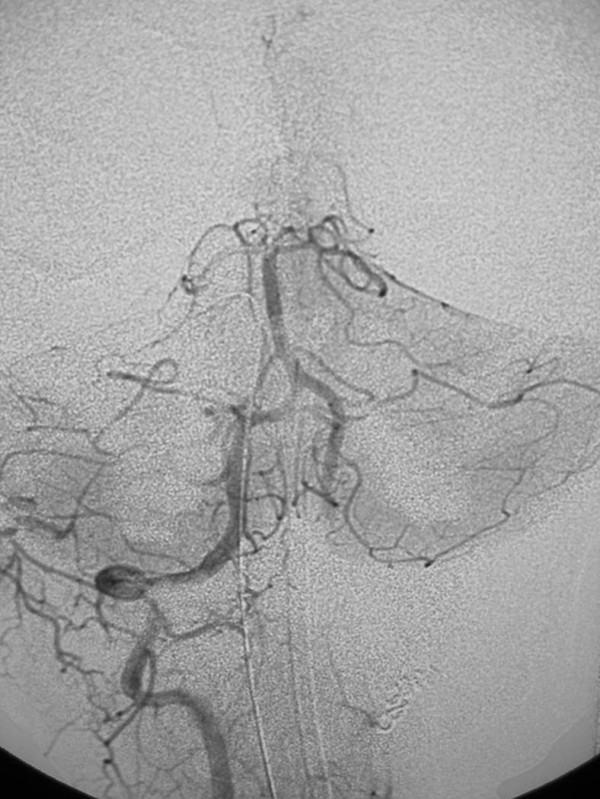
25-year old woman involved in a rollover motor vehicle collision. On admission to the hospital, a screening four-vessel angiogram revealed a pseudoaneurysm of the left vertebral artery at the level of the C1–C2 disc space. Follow-up angiography performed 7 days later revealed enlargement of the pseudoaneurysm and concomitant narrowing of the vertebral artery. Due to the tortuosity of the vertebral artery, stent placement was not deemed a viable option and the vertebral artery was embolized. Post-embolization anteroposterior digital subtraction angiogram, right vertebral artery. There is normal filling of the basilar artery, and reflux of contrast into the distal left vertebral artery which fills the left posterior inferior cerebellar artery (arrow). Images courtesy of Guido Scatorchia, MD.

Contrast enhanced magnetic resonance angiogram demonstrating the arteries and veins of the neck. The entire arterial structures, from the aortic arch to the Circle of Willis, are demonstrated.
References
-
- Lawrence PF, Bell RM, Dayton MT. Essentials of General Surgery. 3. Philadelphia, PA: Williams & Wilkins; 2000.
-
- Fingerhut LA, Warner M. Injury Chartbook. Health, United States, 1996–1997. Hyattsville, MD: National Center for Health Statistics; 1997.
-
- Braunwald E. Harrison's Principles of Internal Medicine. 15. New York, NT: McGraw-Hill; 2001.
-
- Rosenfeld JV, McDermott FT, Laidlaw JD, Cordner SM, Tremayne AB. "The preventability of death in road traffic fatalities with head injury in Victoria, Australia. The Consultative Committee on Road Traffic Fatalities.". J of Clin Neuroscience. 2000;7:507–514. doi: 10.1054/jocn.1999.0694. - DOI - PubMed
-
- Selecki BR, Ring IT, Simpson DA, Vanderfield GK, Sewell MF. "Trauma to the central and peripheral nervous systems: Part I: an overview of mortality, morbidity, and costs; N.S.W. 1977.". Australian and New Zealand Jo of Surg. 1982;52:93–102. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
