

Diagnosis of adenocarcinoma in prostate needle biopsy tissue
- PMID: 17213347
- PMCID: PMC1860598
- DOI: 10.1136/jcp.2005.036442
Diagnosis of adenocarcinoma in prostate needle biopsy tissue
Abstract
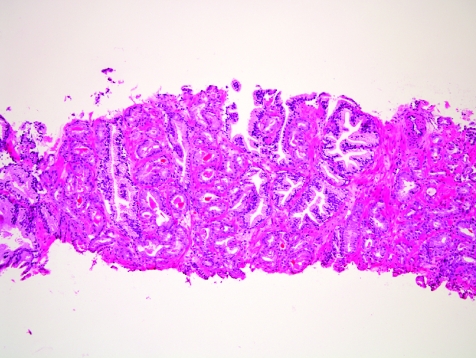
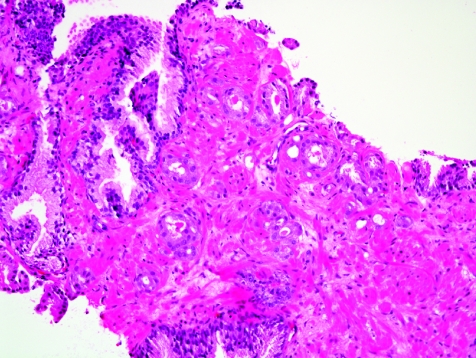
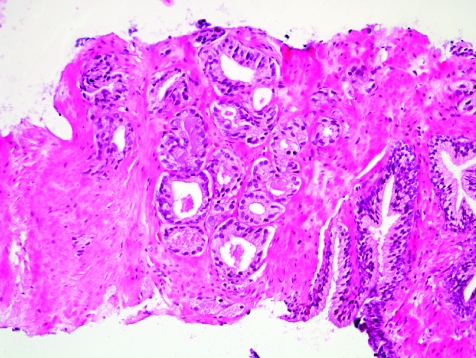
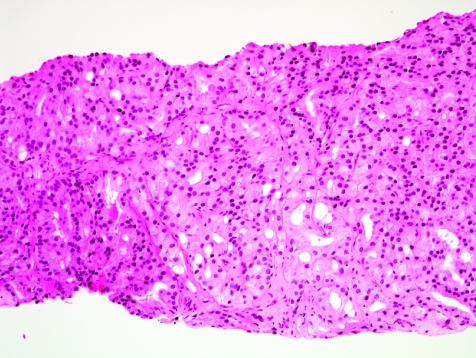
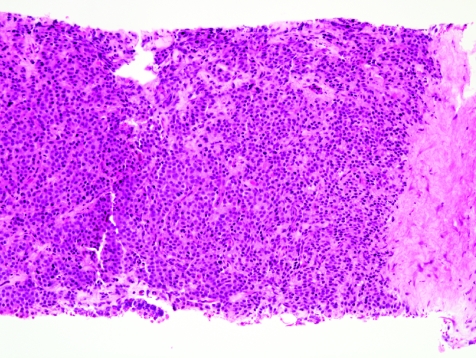
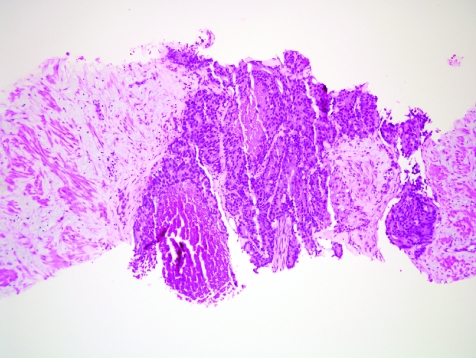
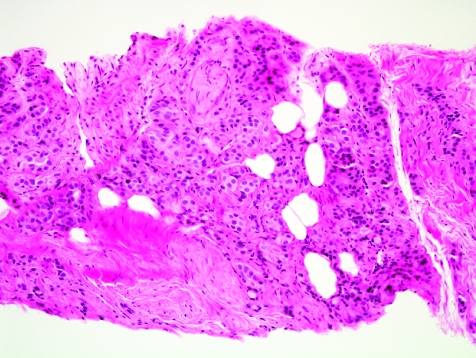
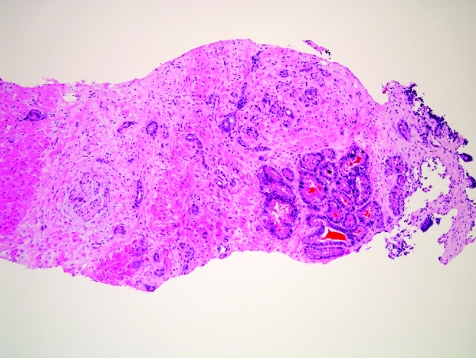
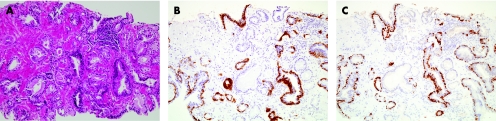
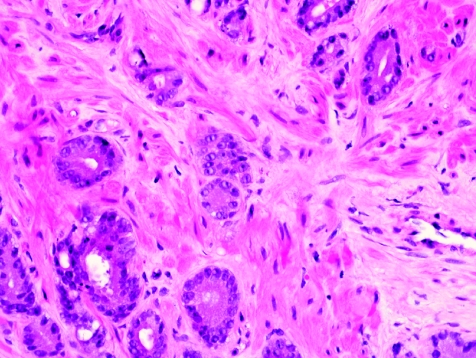
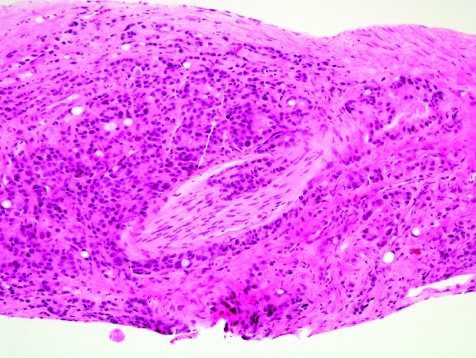
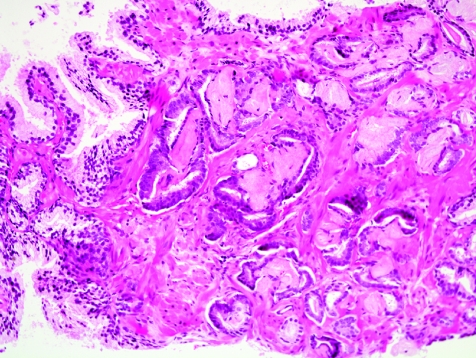
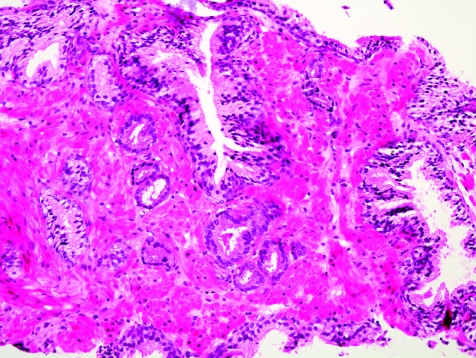
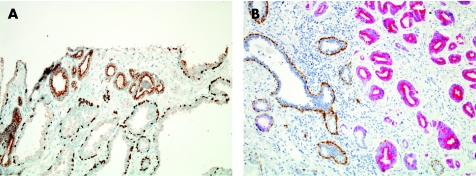
Prostate cancer is a major public health problem throughout the developed world. For patients with clinically localised prostate cancer, the diagnosis is typically established by histopathological examination of prostate needle biopsy samples. Major and minor criteria are used to establish the diagnosis, based on the microscopic appearance of slides stained using haematoxylin and eosin. Major criteria include an infiltrative glandular growth pattern, an absence of basal cells and nuclear atypia in the form of nucleomegaly and nucleolomegaly. In difficult cases, basal cell absence may be confirmed by immunohistochemical stains for high-molecular-weight cytokeratins (marked with antibody 34betaE12) or p63, which are basal cell markers. Minor criteria include intraluminal wispy blue mucin, pink amorphous secretions, mitotic figures, intraluminal crystalloids, adjacent high-grade prostatic intraepithelial neoplasia, amphophilic cytoplasm and nuclear hyperchromasia. Another useful diagnostic marker detectable by immunohistochemistry is alpha-methylacyl coenzyme A racemase (AMACR), an enzyme selectively expressed in neoplastic glandular epithelium. Cocktails of antibodies directed against basal cell markers and AMACR are particularly useful in evaluating small foci of atypical glands, and in substantiating a diagnosis of a minimal adenocarcinoma. Reporting of adenocarcinoma in needle biopsy specimens should always include the Gleason grade and measures of tumour extent in the needle core tissue. Measures of tumour extent are (1) number of cores positive for cancer in the number of cores examined, (2) percentage of needle core tissue affected by carcinoma and (3) linear millimetres of carcinoma present.
Conflict of interest statement
Competing interests: None declared.
References
-
- Parkin D M, Bray F, Ferlay J.et al Global cancer statistics, 2002. CA Cancer J Clin 20055574–108. - PubMed
-
- Humphrey P A. Clinical aspects of prostatic carcinoma, with histopathologic correlations. In: Prostate pathology. Chicago: ASCP Press, 2003226–257.
-
- Epstein J I, Walsh P C, Carmichael M.et al Pathologic and clinical findings to predict tumor extent of nonpalpable (stage T1c) prostate cancer. JAMA 1994271368–374. - PubMed
-
- Berger A P, Spranger R, Kofler K.et al Early detection of prostate cancer with low PSA cut‐off values leads to significant stage migration in radical prostatectomy specimens. Prostate 20035793–98. - PubMed
-
- van der Cruijsen‐Koeter I W, Vis A N, Roobol M J.et al Comparison of screen detected and clinically diagnosed prostate cancer in the European randomized study of screening for prostate cancer, section Rotterdam. J Urol 2005174121–125. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical