

Sacroplasty by CT and fluoroscopic guidance: is the procedure right for your patient?
- PMID: 17213421
- PMCID: PMC8134085
Sacroplasty by CT and fluoroscopic guidance: is the procedure right for your patient?
Abstract
Background and purpose: Sacral insufficiency fractures are an infrequent but often disabling cause of severe low back pain. We report our results of a sacroplasty technique, using CT for needle placement and fluoroscopy to monitor the polymethylmethacrylate injection in a group of patients with sacral insufficiency fractures.
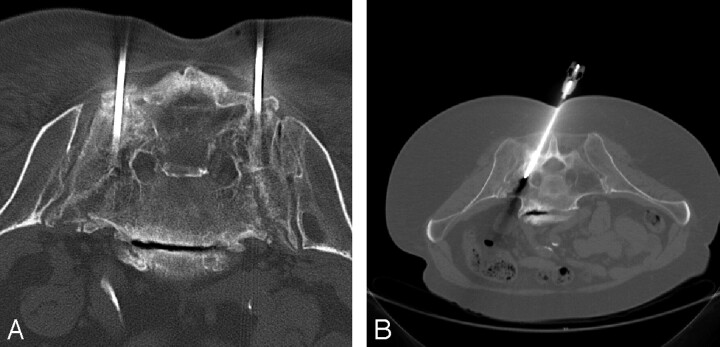
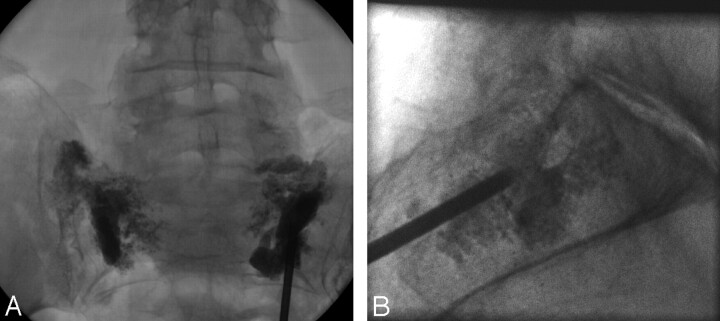
Methods: All patients had a history of chronic back pain and had an osteoporotic sacral insufficiency fracture documented by imaging before the procedure. With the patient under conscious sedation, a bone biopsy needle was placed under CT guidance; the patient was then transferred to the fluoroscopy suite, where a polymethylmethacrylate mixture was injected into the sacrum under real-time fluoroscopy. Clinical outcome was assessed by telephone.
Results: The procedure was performed on 13 female patients with an average age of 76 years (range, 60-88 years). A bilateral procedure was performed in 11 patients and a unilateral procedure was performed in 2 patients. An average of 4.1 mL of cement was injected for each treatment. There were no instances of cement extravasation into the central canal or sacral foramina. Long-term follow-up, averaging 15 months, was available in 6 patients. Five patients (83%) reported no symptoms of pain at all. The final patient, in whom a bilateral procedure was performed, was completely asymptomatic on the left side but reported persistent unilateral pain on the right.
Conclusion: Sacroplasty is a safe and effective procedure in the treatment of sacral insufficiency fractures that can provide substantial pain relief and lead to a better quality of life.
Figures
Similar articles
-
Percutaneous sacroplasty for osteoporotic sacral insufficiency fractures: a prospective, multicenter, observational pilot study.Spine J. 2008 Mar-Apr;8(2):367-73. doi: 10.1016/j.spinee.2007.05.011. Epub 2007 Jul 20. Spine J. 2008. PMID: 17981097
-
Multicenter study to assess the efficacy and safety of sacroplasty in patients with osteoporotic sacral insufficiency fractures or pathologic sacral lesions.J Neurointerv Surg. 2013 Sep 1;5(5):461-6. doi: 10.1136/neurintsurg-2012-010347. Epub 2012 Jun 8. J Neurointerv Surg. 2013. PMID: 22684691
-
Sacroplasty: a treatment for sacral insufficiency fractures.AJNR Am J Neuroradiol. 2003 May;24(5):1003-7. AJNR Am J Neuroradiol. 2003. PMID: 12748113 Free PMC article.
-
Safety and Efficacy of Sacroplasty for Sacral Fractures: A Systematic Review and Meta-Analysis.J Vasc Interv Radiol. 2019 Nov;30(11):1845-1854. doi: 10.1016/j.jvir.2019.06.013. Epub 2019 Oct 3. J Vasc Interv Radiol. 2019. PMID: 31587952
-
[Osteoporotic sacral fracture--a painful condition, easy to miss. Sacroplasty a new treatment with quick pain relief].Lakartidningen. 2010 Feb 3-9;107(5):251-4. Lakartidningen. 2010. PMID: 20297565 Review. Swedish. No abstract available.
Cited by
-
Safety and effectiveness of percutaneous sacroplasty: a single-centre experience in 58 consecutive patients with tumours or osteoporotic insufficient fractures treated under fluoroscopic guidance.Eur Radiol. 2013 Oct;23(10):2764-72. doi: 10.1007/s00330-013-2881-3. Epub 2013 May 21. Eur Radiol. 2013. PMID: 23689309 Clinical Trial.
-
Sacroplasty for cancer-associated insufficiency fractures.Neurosurgery. 2015 Apr;76(4):446-50; discussion 450. doi: 10.1227/NEU.0000000000000658. Neurosurgery. 2015. PMID: 25635890 Free PMC article.
-
Percutaneous sacroplasty for sacral metastatic tumors under fluoroscopic guidance only.Korean J Radiol. 2008 Nov-Dec;9(6):572-6. doi: 10.3348/kjr.2008.9.6.572. Korean J Radiol. 2008. PMID: 19039277 Free PMC article.
-
CT fluoroscopy-guided percutaneous vertebroplasty in spinal malignancy: technical results, PMMA leakages, and complications in 202 patients.Skeletal Radiol. 2012 Nov;41(11):1391-400. doi: 10.1007/s00256-012-1365-x. Skeletal Radiol. 2012. PMID: 22286549
-
Percutaneous sacroplasty with the use of C-arm flat-panel detector CT: technical feasibility and clinical outcome.Skeletal Radiol. 2011 Apr;40(4):453-60. doi: 10.1007/s00256-010-0959-4. Epub 2010 May 15. Skeletal Radiol. 2011. PMID: 20473493
References
-
- Brook AL, Mirsky DM, Bello JA. Computerized tomography guided sacroplasty: a practical treatment for sacral insufficiency fracture. Spine 2005;15:E450–54 - PubMed
-
- Deen H, Nottmeier E. Balloon kyphoplasty for treatment of sacral insufficiency fractures. Neurosurg Focus 2005;3:1–5 - PubMed
-
- Garant M. Sacroplasty: a new treatment for sacral insufficiency fracture. J Vasc Interv Radiol 2002;13:1265–67 - PubMed
-
- Leroux JL, Denat B, Thomas E, et al. Sacral insufficiency fractures presenting as acute low-back pain biomechanical aspects. Spine 1993;18:2505–06 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical