

Vertebral osteonecrosis: MR imaging findings and related changes on adjacent levels
- PMID: 17213422
- PMCID: PMC8134120
Vertebral osteonecrosis: MR imaging findings and related changes on adjacent levels
Abstract
Background and purpose: No prior report has comprehensively discussed the intravertebral vacuum cleft sign and the fluid sign on MR images of vertebral osteonecrosis. The purpose of this study was to investigate MR images of osteonecrotic vertebral bodies and adjacent intervertebral disks and vertebral bodies.
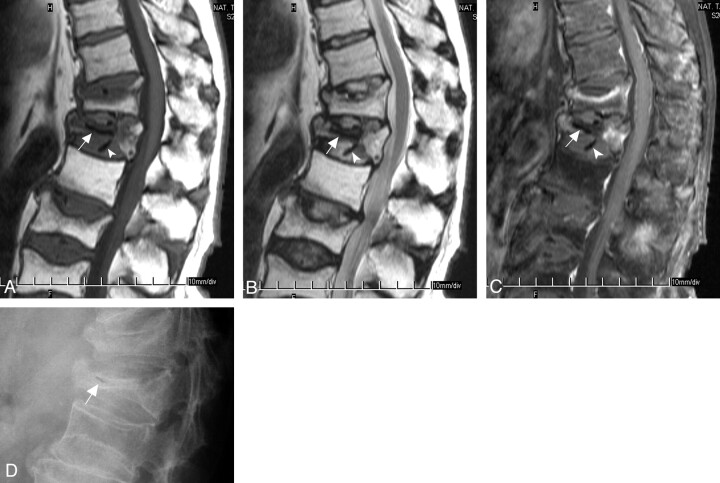
Methods: We retrospectively reviewed MR images of patients with vertebral osteonecrosis. Affected vertebral bodies with osteonecrosis were defined as an avascular area (nonenhanced area on enhanced T1-weighted images) with collections of intravertebral fluid (hyperintense signal on T2-weighted images), air (signal void on all images), or both. The degree of vertebral collapse was classified as mild (>50%) or severe (<50%) preserved vertebral height. Changes in adjacent intervertebral disks or vertebral bodies 2 above and 2 below the affected vertebrae were compared.
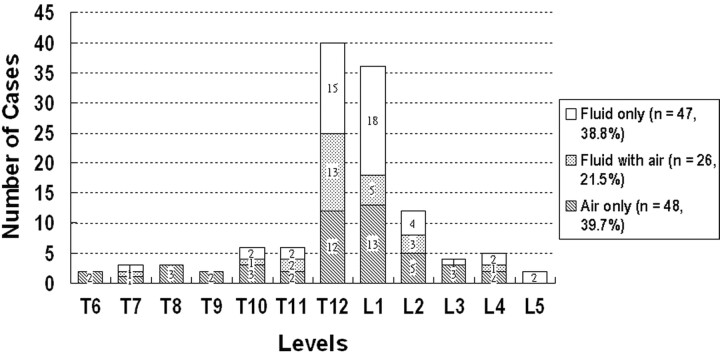
Results: We enrolled 112 patients (30 men, 82 women; 121 vertebral bodies) in our study. Intravertebral air alone was observed in 48 involved levels (39.7%), intravertebral fluid alone was found in 47 (38.8%), and both coexisted in 26 (21.5%). Degree of vertebral collapse in affected vertebral bodies significantly differed with presence of air or fluid (P < .05). Vertebral compression fractures adjacent to the affected vertebral bodies were more common in those with intravertebral air alone than in those with intravertebral fluid alone (P < .05).
Conclusion: Vertebral collapse was more advanced and adjacent vertebral compression fractures were more frequent in patients with intravertebral air than in those with intravertebral fluid.
Figures


Similar articles
-
The intravertebral vacuum phenomenon ("vertebral osteonecrosis"). Migration of intradiscal gas in a fractured vertebral body?Spine (Phila Pa 1976). 1997 Aug 15;22(16):1885-91. doi: 10.1097/00007632-199708150-00015. Spine (Phila Pa 1976). 1997. PMID: 9280025
-
Avascular necrosis of the vertebral body: MR imaging.Radiology. 1989 Jul;172(1):219-22. doi: 10.1148/radiology.172.1.2740507. Radiology. 1989. PMID: 2740507
-
Are intravertebral vacuum phenomena benign lesions?Eur Spine J. 2011 Aug;20(8):1341-8. doi: 10.1007/s00586-011-1789-3. Epub 2011 Apr 30. Eur Spine J. 2011. PMID: 21533599 Free PMC article. Review.
-
Acute osteoporotic and neoplastic vertebral compression fractures: fluid sign at MR imaging.Radiology. 2002 Dec;225(3):730-5. doi: 10.1148/radiol.2253011413. Radiology. 2002. PMID: 12461253
-
Intravertebral vacuum cleft sign: a cause of vertebral cold defect on bone scan.Skeletal Radiol. 2016 May;45(5):707-12. doi: 10.1007/s00256-016-2331-9. Epub 2016 Jan 13. Skeletal Radiol. 2016. PMID: 26758604 Review.
Cited by
-
Avascular necrosis: radiological findings and main sites of involvement - pictorial essay.Radiol Bras. 2019 May-Jun;52(3):187-192. doi: 10.1590/0100-3984.2017.0151. Radiol Bras. 2019. PMID: 31210694 Free PMC article.
-
Efficacy and safety of hollow pedicle screw-anchored bone cement combined with posterior long-segment fixation for Stage III Kümmell's disease.Jt Dis Relat Surg. 2025 Jan 2;36(1):15-23. doi: 10.52312/jdrs.2024.1834. Epub 2024 Nov 22. Jt Dis Relat Surg. 2025. PMID: 39719897 Free PMC article.
-
Posterior Fixation Combined with Vertebroplasty or Vertebral Column Resection for the Treatment of Osteoporotic Vertebral Compression Fractures with Intravertebral Cleft Complicated by Neurological Deficits.Biomed Res Int. 2019 Dec 14;2019:4126818. doi: 10.1155/2019/4126818. eCollection 2019. Biomed Res Int. 2019. PMID: 31915692 Free PMC article.
-
Revisiting Kümmell's disease: MRI findings beyond the intraosseous cavity for improved diagnosis.Neuroradiology. 2022 Aug;64(8):1681-1688. doi: 10.1007/s00234-022-02976-z. Epub 2022 May 17. Neuroradiology. 2022. PMID: 35577995
-
Bone microarchitecture and metabolism in elderly male patients with signs of intravertebral cleft on MRI.Eur Radiol. 2022 Jun;32(6):3931-3943. doi: 10.1007/s00330-021-08458-9. Epub 2022 Jan 6. Eur Radiol. 2022. PMID: 34989849
References
-
- Theodorou DJ. The intravertebral vacuum cleft sign. Radiology 2001;21:787–88 - PubMed
-
- Malghem J, Maldague B, Labaisse M. Intravertebral vacuum cleft: changes in content after supine positioning. Radiology 1993;187:483–87 - PubMed
-
- Naul LG, Peet GJ, Maupin WB. Avascular necrosis of the vertebral body. Radiology 1989;172:219–22 - PubMed
-
- Dupuy DE, Palmer WE, Rosenthal DI. Vertebral fluid collection associated with vertebral collapse. AJR Am J Roentgenol 1996;167:1535–38 - PubMed
-
- Baur A, Stabler A, Arbogast S, et al. Acute osteoporotic and neoplastic vertebral compression fractures: fluid sign at MR imaging. Radiology 2002;225:730–35 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical