

Detection and characterization of intracranial aneurysms with 16-channel multidetector row CT angiography: a prospective comparison of volume-rendered images and digital subtraction angiography
- PMID: 17213425
- PMCID: PMC8134101
Detection and characterization of intracranial aneurysms with 16-channel multidetector row CT angiography: a prospective comparison of volume-rendered images and digital subtraction angiography
Abstract
Background and purpose: The aim of our study was to compare multidetector row CT angiography (MDCTA) with digital subtraction angiography (DSA) in the detection and characterization of intracranial aneurysms.
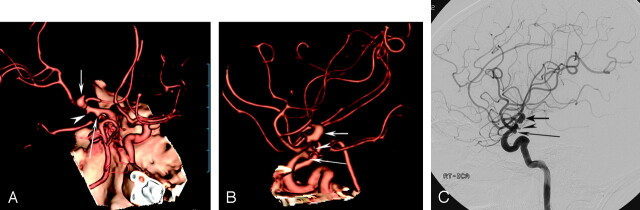
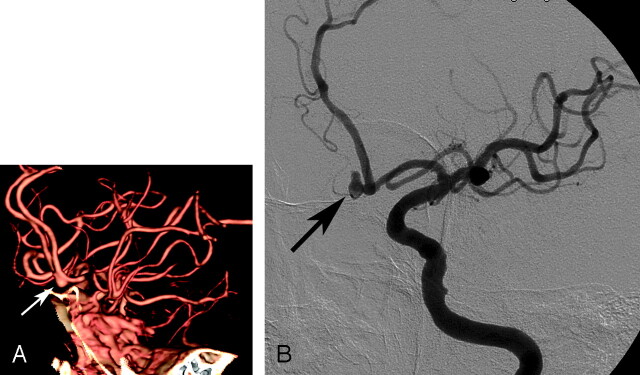
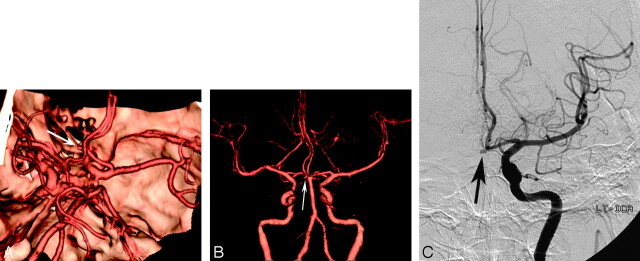
Materials and methods: In our blinded prospective study, 85 patients with suspected intracranial aneurysm (47 women, 38 men; age range, 19-83 years) underwent both 16-channel MDCTA and DSA. The MDCT angiograms were interpreted for the presence, location, size, ratio of the neck to the dome (N/D ratio), and lobularity of the aneurysms and relationship of the aneurysm with the adjacent arterial branches, by using volume-rendering techniques. MDCTA and DSA images (reference standard) were interpreted by 2 independent readers, and the results were compared.
Results: A total of 93 aneurysms were detected at DSA in 71 patients, whereas no aneurysms were detected in 14 patients. Compared with DSA, the overall sensitivity, specificity, and accuracy of MDCTA on a per-aneurysm basis were 92.5%, 93.3%, and 92.6%, respectively, for both independent readers. For aneurysms of <3 mm, however, MDCTA had a sensitivity of 74.1% for reader 1 and 77.8% for reader 2. There was excellent agreement between readers in the detection of aneurysms (kappa = 0.822). In addition, MDCTA was also accurate in determining N/D ratio of aneurysms, aneurysm lobularity, and adjacent arterial branches.
Conclusion: MDCTA is accurate in the detection and characterization of intracranial aneurysms and can be used as a reliable alternative imaging technique to DSA in selected cases.
Figures
Similar articles
-
Detection and evaluation of intracranial aneurysms with 16-row multislice CT angiography: comparison with conventional angiography.Emerg Radiol. 2008 Sep;15(5):311-6. doi: 10.1007/s10140-008-0727-0. Epub 2008 May 8. Emerg Radiol. 2008. PMID: 18463904
-
Performance analysis of 8-channel MDCT angiography in detection, localization, and sizing of intracranial aneurysms identified on DSA.Diagn Interv Radiol. 2009 Jun;15(2):81-5. Diagn Interv Radiol. 2009. PMID: 19517376
-
Multidetector-row CT angiography of cerebral vasospasm after aneurysmal subarachnoid hemorrhage: comparison of volume-rendered images and digital subtraction angiography.AJNR Am J Neuroradiol. 2006 Feb;27(2):370-7. AJNR Am J Neuroradiol. 2006. PMID: 16484413 Free PMC article.
-
Dangerous advances in measurements from digital subtraction angiography: when is a millimeter not a millimeter?AJNR Am J Neuroradiol. 2009 Mar;30(3):459-61. doi: 10.3174/ajnr.A1381. Epub 2008 Nov 27. AJNR Am J Neuroradiol. 2009. PMID: 19039047 Free PMC article. Review.
-
State-of-the-art 3DCT angiography assessment of lower extremity trauma: typical findings, pearls, and pitfalls.Emerg Radiol. 2013 Jun;20(3):175-84. doi: 10.1007/s10140-012-1094-4. Epub 2012 Nov 27. Emerg Radiol. 2013. PMID: 23184446 Review.
Cited by
-
Value of CT angiography for the detection of intracranial vascular lesions in patients with acute severe headache.Eur Radiol. 2013 Jun;23(6):1443-9. doi: 10.1007/s00330-012-2751-4. Epub 2012 Dec 21. Eur Radiol. 2013. PMID: 23263605
-
Presurgical planning for arteriovenous malformations using multidetector row CT.Neurosurg Rev. 2012 Jul;35(3):393-9; discussion 399-400. doi: 10.1007/s10143-012-0383-4. Epub 2012 Mar 23. Neurosurg Rev. 2012. PMID: 22437568
-
Diagnostic accuracy of CT angiography with matched mask bone elimination for detection of intracranial aneurysms: comparison with digital subtraction angiography and 3D rotational angiography.AJNR Am J Neuroradiol. 2008 Jan;29(1):134-9. doi: 10.3174/ajnr.A0741. Epub 2007 Oct 10. AJNR Am J Neuroradiol. 2008. PMID: 17928381 Free PMC article.
-
Diagnostic Impact of Bone-Subtraction CT Angiography for Patients with Acute Subarachnoid Hemorrhage.AJNR Am J Neuroradiol. 2016 Feb;37(2):236-43. doi: 10.3174/ajnr.A4497. Epub 2015 Oct 8. AJNR Am J Neuroradiol. 2016. PMID: 26450538 Free PMC article.
-
Comparison of 2D digital subtraction angiography and 3D rotational angiography in the evaluation of dome-to-neck ratio.AJNR Am J Neuroradiol. 2009 Apr;30(4):831-4. doi: 10.3174/ajnr.A1444. Epub 2009 Jan 8. AJNR Am J Neuroradiol. 2009. PMID: 19131410 Free PMC article.
References
-
- King JT Jr. Epidemiology of aneurysmal subarachnoid hemorrhage. Neuroimaging Clin N Am 1997;7:659–68 - PubMed
-
- Cloft HJ, Joseph GJ, Dion JE. Risk of cerebral angiography in patients with subarachnoid hemorrhage, cerebral aneurysm, and arteriovenous malformation: a meta-analysis. Stroke 1999;30:317–20 - PubMed
-
- Hankey GJ, Wrlow CP, Sellar RJ. Cerebral angiographic risk in mild cerebrovascular disease. Stroke 1990;21:209–22 - PubMed
-
- Ronkainen A, Puranen M, Hernesniemi JA, et al. Intracranial aneurysms: MR angiographic screening in 400 asymptomatic individuals with increased familial risk. Radiology 1995;195:35–40 - PubMed
-
- Wiebers DO, Torres VE. Screening for unruptured intracranial aneurysms in autosomal-dominant polycystic kidney disease. N Engl J Med 1992;327:953–55 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical