

CT angiographic analysis of carotid artery stenosis: comparison of manual assessment, semiautomatic vessel analysis, and digital subtraction angiography
- PMID: 17213433
- PMCID: PMC8134104
CT angiographic analysis of carotid artery stenosis: comparison of manual assessment, semiautomatic vessel analysis, and digital subtraction angiography
Abstract
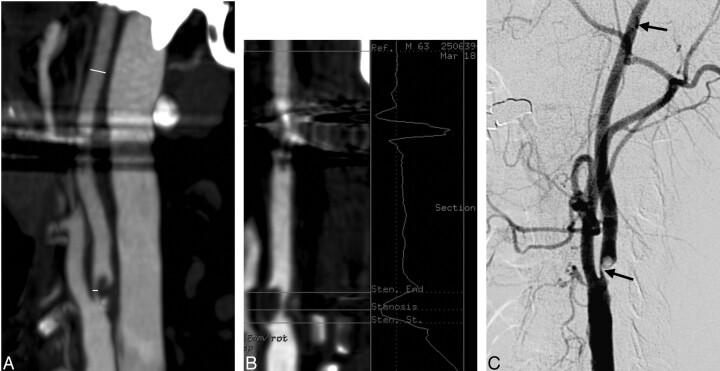
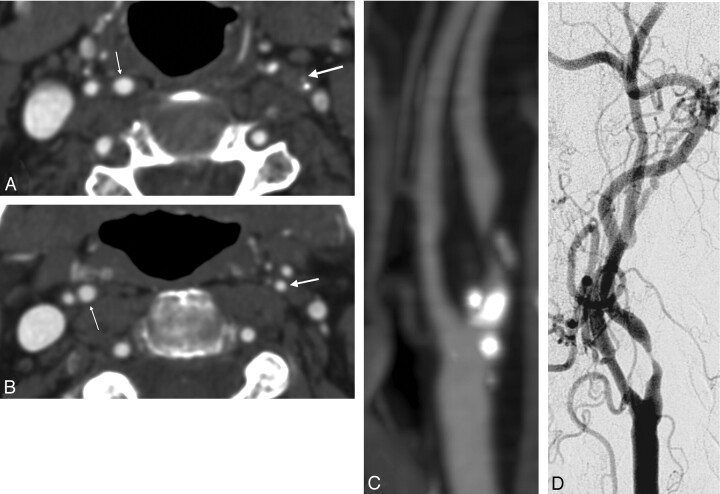
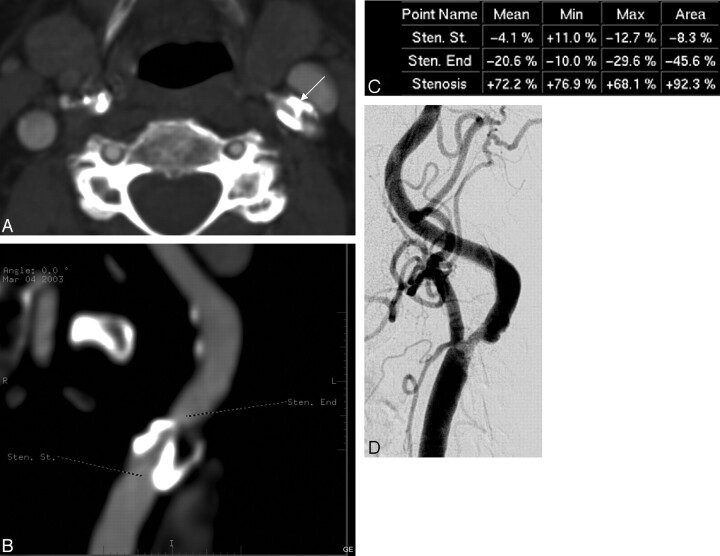
Background and purpose: To compare multisection CT angiography (CTA) analyzed with source/maximum intensity projection (MIP) images as well as semiautomated vessel analysis software with intra-arterial digital subtraction angiography (DSA) in detection and grading of carotid artery bifurcation stenosis.
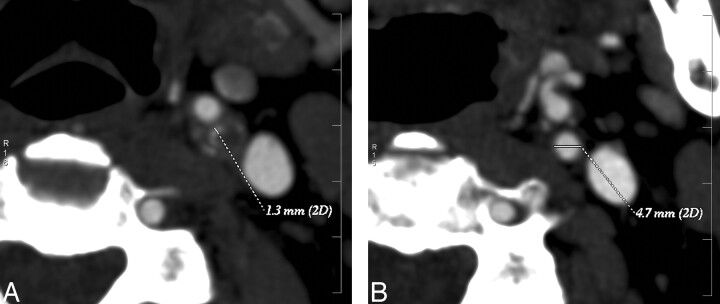
Methods: Consecutive patients with sonography evidence of a marked internal carotid artery stenosis underwent both carotid CTA and DSA (37 patients, 73 vessels). In CTA, the grade of stenosis was determined using axial source and MIP images as well as vessel analysis. The scans were blind-analyzed by 2 neuroradiologists using the NASCET criteria.
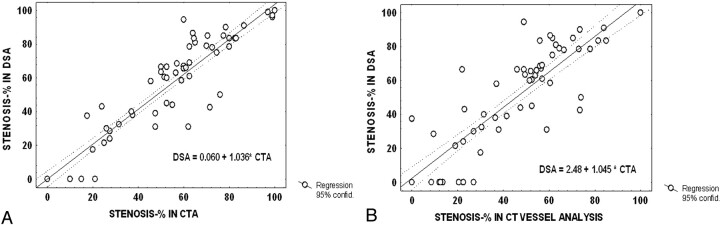
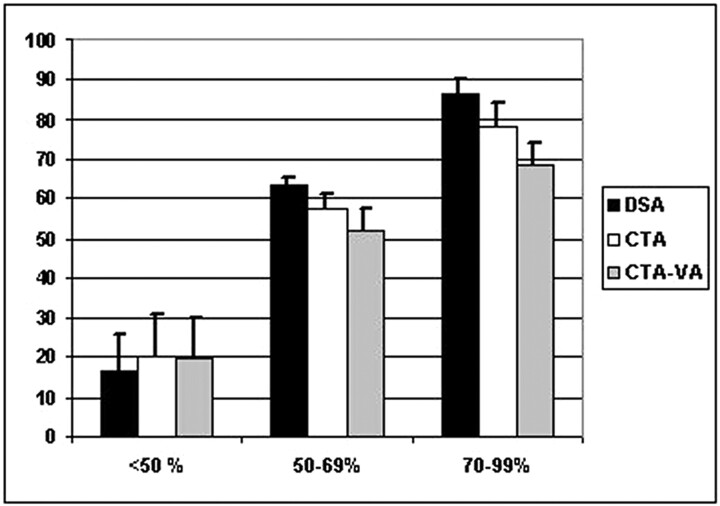
Results: Correlation of CTA source/MIP images versus DSA estimates of stenosis (R = 0.95) was higher than for the vessel analysis method versus DSA (R = 0.89). Compared with DSA, CTA source/MIP images underestimated high (78.2% versus 86.4%, P < .05) and moderate grades of stenosis (57.3% versus 63.1%, P < .05) to a lesser extent than the vessel analysis method (68.5% versus 83.5% and 51.8% versus 63.1%, P < .05). For a high-grade stenosis, sensitivity and specificity of source/MIP image CTA were 75% and 96%, respectively, whereas for the vessel analysis method, they were 47% and 96%, respectively. For moderate stenosis, the source/MIP image CTA sensitivity and specificity were 88% and 82%, respectively, and for vessel analysis method, 62% and 82%, respectively. CTA detected all 4 occlusions.
Conclusion: In evaluation of carotid stenosis, CTA provides an adequate, less invasive alternative with a high correlation to conventional DSA, though it tends to underestimate clinically relevant grades of stenosis. Its accuracy is not improved by semiautomated analysis. The data support the use of CTA in confirming carotid occlusion.
Figures
References
-
- Bonita R. Epidemiology of stroke. Lancet 1992;339:342–44 - PubMed
-
- Bamford J, Sandercock P, Dennis M, et al. Classification and natural history of clinically identifiable subtypes of cerebral infarction. Lancet 1991;337:1521–26 - PubMed
-
- Anonymous. Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med 1991;325:445–53 - PubMed
-
- Warlow C. MRC European Carotid Surgery Trial: interim results for symptomatic patients with severe (70–99%) or with mild (0–29%) carotid stenosis. Lancet 1991;337:1235–43 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical