

Carotid blowout syndrome in patients with head-and-neck cancers: reconstructive management by self-expandable stent-grafts
- PMID: 17213454
- PMCID: PMC8134086
Carotid blowout syndrome in patients with head-and-neck cancers: reconstructive management by self-expandable stent-grafts
Abstract
Background and purpose: Some reports of reconstructive management of carotid blowout syndrome (CBS) with stent-grafts are promising, but some are unfavorable. This study sought to evaluate the hemostatic efficacy, safety, and outcome of reconstructive, endovascular stent-graft placement in patients with head-and-neck cancers in association with CBS.
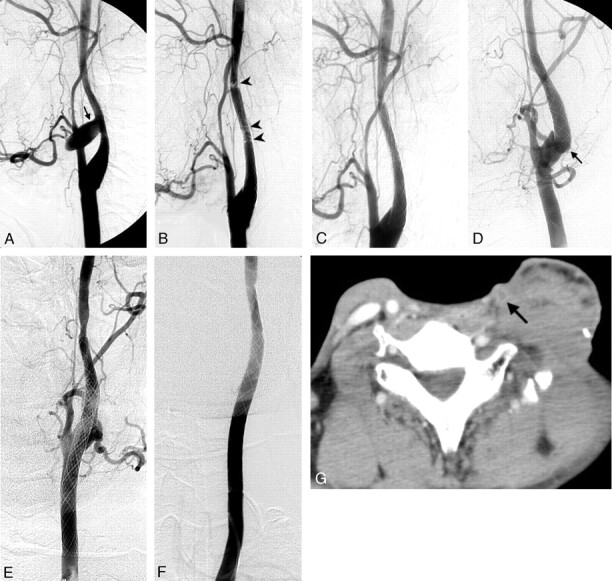
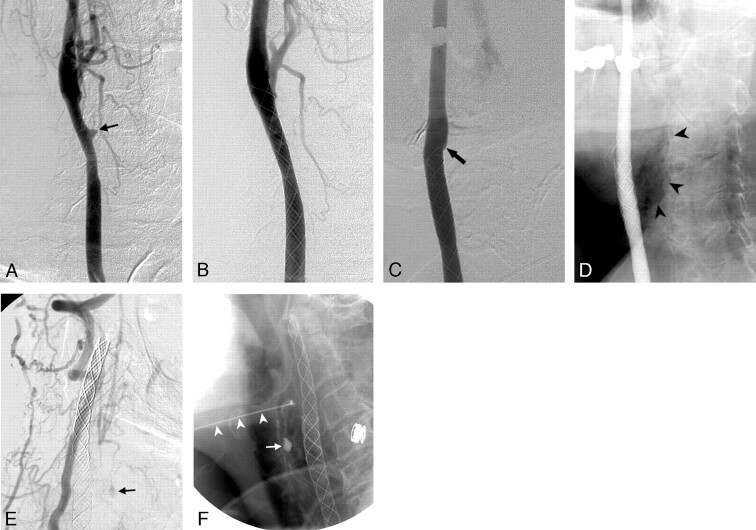
Methods: Eight patients with head-and-neck cancers with CBS were treated with self-expandable stent-grafts. We evaluated the initial hemostatic results, complications, and outcomes by assessing the clinical and imaging findings.
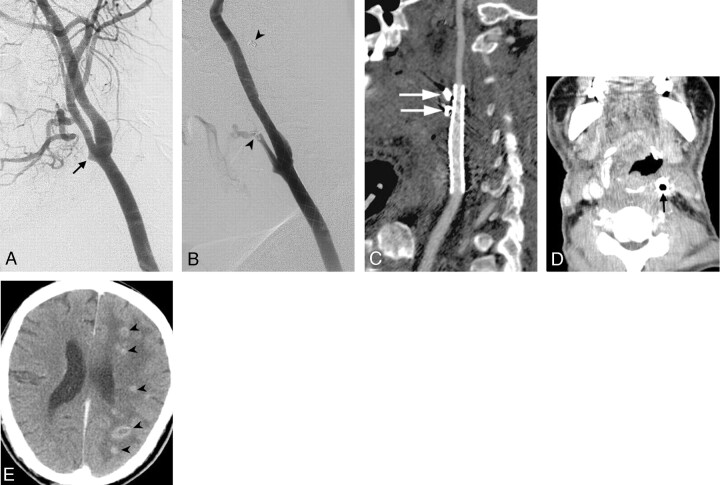
Results: Immediate hemostasis was achieved in all patients. Initial complications included stroke in 1 patient and asymptomatic thrombosis of the carotid artery in 2 patients. Delayed complications included rebleeding, delayed carotid thrombosis, and brain abscess formation. Rebleeding was noted in 4 patients and was successfully managed with a second stent-graft and embolization in 2 of them. Delayed carotid thrombosis with follow-up after 3 months was found in 3 patients, 1 of whom had associated brain abscesses.
Conclusion: Although stent-grafts achieved immediate and initial hemostasis in patients with head-and-neck cancers and CBS, long-term safety, stent patency, and permanency of hemostasis appeared unfavorable. This treatment may be for temporary or emergency purposes rather than serving as a permanent measure. We suggest its applications in patients with acute CBS that precludes performance of an occlusion test, as well as when carotid occlusion poses an unusually high risk of neurologic morbidity. We also propose prophylactic antibiotic treatment and combined embolization of pathologic vascular feeders to improve outcomes.
Figures

References
-
- Macdonald S, Gan J, Mckay AJ, et al. Endovascular treatment of acute carotid blowout syndrome. J Vasc Interv Radiol 2000;11:1184–88 - PubMed
-
- Citardi MJ, Chaloupak JC, Son YH, et al. Management of carotid artery rupture by monitored endovascular therapeutic occlusion (1988–1994). Laryngoscope 1995;105:1086–92 - PubMed
-
- Warren FM, Cohen JI, Nesbit GM, et al. Management of carotid “blowout” with endovascular stent grafts. Laryngoscope 2002;112:428–33 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical