

Successful treatment of cervical myelopathy with minimal morbidity by circumferential decompression and fusion
- PMID: 17216528
- PMCID: PMC2200762
- DOI: 10.1007/s00586-006-0291-9
Successful treatment of cervical myelopathy with minimal morbidity by circumferential decompression and fusion
Abstract
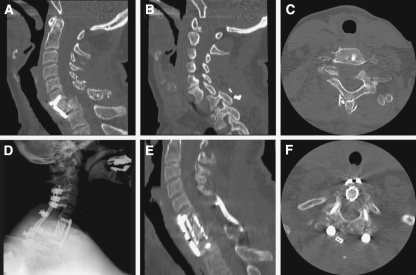
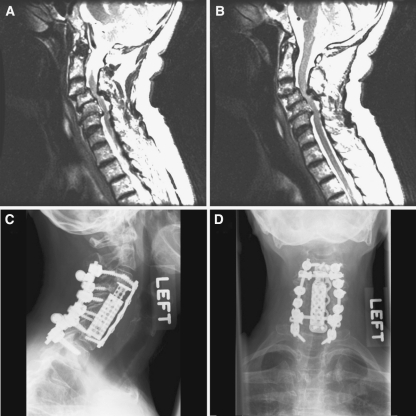
Circumferential cervical decompression and fusion (CCDF) is an important technique for treating patients with severe cervical myelopathy. While circumferential cervical decompression and fusion may provide improved spinal cord decompression and stability compared to unilateral techniques, it is commonly associated with increased morbidity and mortality. We performed a retrospective analysis of patients undergoing CCDF at the University of California, San Francisco (UCSF) between January 2003 and December 2004. We identified 53 patients and reviewed their medical records to determine the effectiveness of CCDF for improving myelopathy, pain, and neurological function. Degree of fusion, functional anatomic alignment, and stability were also assessed. Operative morbidity and mortality were measured. The most common causes of cervical myelopathy, instability, or deformity were degenerative disease (57%) and traumatic injury (34%). Approximately one-fifth of patients had a prior fusion performed elsewhere and presented with fusion failure or adjacent-level degeneration. Postoperatively, all patients had stable (22.6%) or improved (77.4%) Nurick grades. The average preoperative and postoperative Nurick grades were 2.1 +/- 1.9 and 0.4 +/- 0.9, respectively. Pain improved in 85% of patients. All patients had radiographic evidence of fusion at last follow-up. The most common complication was transient dysphagia. Our average clinical follow-up was 27.5 +/- 9.5 months. We present an extensive series of patients and demonstrate that cervical myelopathy can successfully be treated with CCDF with minimal operative morbidity. CCDF may provide more extensive decompression of the spinal cord and may be more structurally stable. Concerns regarding operation-associated morbidity should not strongly influence whether CCDF is performed.
Figures
Similar articles
-
Clinical results and complications of circumferential spinal cord decompression through a single posterior approach for thoracic myelopathy caused by ossification of posterior longitudinal ligament.Spine (Phila Pa 1976). 2008 May 15;33(11):1199-208. doi: 10.1097/BRS.0b013e3181714515. Spine (Phila Pa 1976). 2008. PMID: 18469693
-
[Systematic circumferential (360 degree) decompression treatment of major arthrotic cervical stenosis].Rev Chir Orthop Reparatrice Appar Mot. 2002 Sep;88(5):449-59. Rev Chir Orthop Reparatrice Appar Mot. 2002. PMID: 12399709 French.
-
[Treatment of cervical spondylotic myelopathy by decompression of spinal canal and internal fixation with the combination of anterior and posterior approaches].Zhonghua Yi Xue Za Zhi. 2007 Jan 2;87(1):28-31. Zhonghua Yi Xue Za Zhi. 2007. PMID: 17403308 Chinese.
-
Indications for circumferential surgery for cervical spondylotic myelopathy.Spine J. 2006 Nov-Dec;6(6 Suppl):299S-307S. doi: 10.1016/j.spinee.2006.04.025. Spine J. 2006. PMID: 17097550 Review.
-
Posterior plating of the cervical spine.J Spinal Disord. 1995 Apr;8(2):111-5. J Spinal Disord. 1995. PMID: 7606116 Review.
Cited by
-
Construct stability of an instrumented 2-level cervical corpectomy model following fatigue testing: biomechanical comparison of circumferential antero-posterior instrumentation versus a novel anterior-only transpedicular screw-plate fixation technique.Eur Spine J. 2015 Dec;24(12):2848-56. doi: 10.1007/s00586-015-3770-z. Epub 2015 Jan 23. Eur Spine J. 2015. PMID: 25612849
-
Biomechanical testing of circumferential instrumentation after cervical multilevel corpectomy.Eur Spine J. 2015 Dec;24(12):2788-98. doi: 10.1007/s00586-015-4167-8. Epub 2015 Aug 2. Eur Spine J. 2015. PMID: 26233243
-
Different Approaches for Treating Multilevel Cervical Spondylotic Myelopathy: A Retrospective Study of 153 Cases from a Single Spinal Center.PLoS One. 2015 Oct 13;10(10):e0140031. doi: 10.1371/journal.pone.0140031. eCollection 2015. PLoS One. 2015. PMID: 26460488 Free PMC article.
-
Pars interarticularis screws for posterior cervical fusion - investigating a new trajectory using a CT-based multiplanar reconstruction: Part I.Acta Neurochir (Wien). 2024 Jul 11;166(1):295. doi: 10.1007/s00701-024-06184-x. Acta Neurochir (Wien). 2024. PMID: 38990411 Free PMC article.
-
Expansive open-door laminoplasty and selective anterior cervical decompression and fusion for treatment of multilevel cervical spondylotic myelopathy.Orthop Surg. 2011 Aug;3(3):161-6. doi: 10.1111/j.1757-7861.2011.00143.x. Orthop Surg. 2011. PMID: 22009646 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
