

Comparison of an interferon-gamma release assay with tuberculin skin testing in HIV-infected individuals
- PMID: 17218620
- PMCID: PMC1899289
- DOI: 10.1164/rccm.200608-1088OC
Comparison of an interferon-gamma release assay with tuberculin skin testing in HIV-infected individuals
Abstract
Rationale: Although interferon (IFN)-gamma release assays are approved for the diagnosis of latent tuberculosis infection (LTBI), limited data exist regarding their performance in HIV infection.
Objectives: To compare tuberculin skin test (TST) results to the commercial IFN-gamma release assay QuantiFERON-TB Gold In-Tube (QFT) for the diagnosis of LTBI in HIV-infected adults.
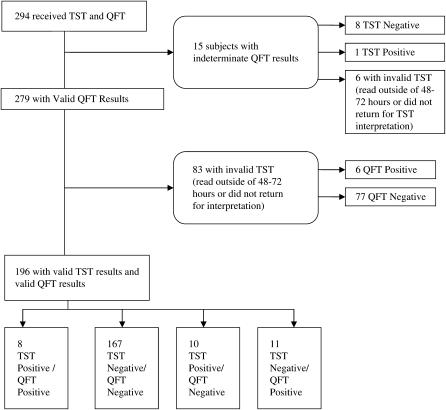
Methods: A total of 294 HIV-infected subjects sampled from two San Francisco cohorts underwent TST, using 5 TU of purified protein derivative, and QFT, measuring IFN-gamma response to Mycobacterium tuberculosis-specific RD-1 antigens.
Main results: Of 294 participants, 205 (70%) returned for an evaluable TST. Concordance between QFT and TST was 89.3% (kappa=0.37, p=0.007). However, in subjects with positive test results by either TST or QFT, only 28% (8/29) had positive test results by both modalities. TST-positive/QFT-negative discordant results were found in 5.1% of subjects and TST-negative/QFT-positive discordance in 5.6%. Indeterminate QFT results occurred in 5.1%, all due to a failure to respond to the phytohemagglutinin-positive control. Subjects with a CD4(+) count of less than 100 cells/mm(3) had a relative risk of an indeterminate result of 4.24 (95% confidence interval, 1.55-11.61; p=0.003) compared with those with a CD4(+) count of 100 or more.
Conclusions: Overall concordance between QFT and TST in HIV infection was high, but agreement among subjects with positive tests by either modality was low.
Figures
References
-
- World Health Organization. Two diseases: one patient. Report of the Third Global TB/HIV Working Group meeting. Geneva, Switzerland: World Health Organization; 2003.
-
- Lawn SD, Bekker LG, Wood R. How effectively does HAART restore immune responses to Mycobacterium tuberculosis? Implications for tuberculosis control. AIDS 2005;19:1113–1124. - PubMed
-
- Chaisson RE, Keruly JC, McAvinue S, Gallant JE, Moore RD. Effects of an incentive and education program on return rates for PPD test reading in patients with HIV infection. J Acquir Immune Defic Syndr Hum Retrovirol 1996;11:455–459. - PubMed
-
- Caiaffa WT, Graham NM, Galai N, Rizzo RT, Nelson KE, Vlahov D. Instability of delayed-type hypersensitivity skin test anergy in human immunodeficiency virus infection. Arch Intern Med 1995;155:2111–2117. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
