

Accuracy of the bedside head impulse test in detecting vestibular hypofunction
- PMID: 17220287
- PMCID: PMC2117540
- DOI: 10.1136/jnnp.2006.109512
Accuracy of the bedside head impulse test in detecting vestibular hypofunction
Erratum in
- J Neurol Neurosurg Psychiatry. 2008 Aug;79(8):967
Abstract
Objective: To determine the accuracy of the bedside head impulse test (bHIT) by direct comparison with results from the quantitative head impulse test (qHIT) in the same subjects, and to investigate whether bHIT sensitivity and specificity changes with neuro-otological training.
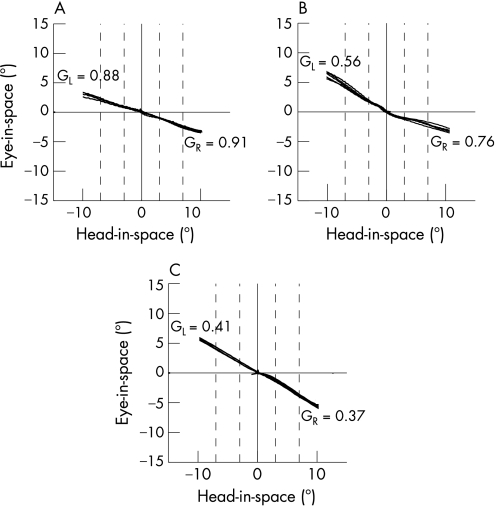
Methods: Video clips of horizontal bHIT to both sides were produced in patients with unilateral and bilateral peripheral vestibular deficits (n = 15) and in healthy subjects (n = 9). For qHIT, eye and head movements were recorded with scleral search coils on the right eye and the forehead. Clinicians (neurologists or otolaryngologists) with at least 6 months of neuro-otological training ("experts": n = 12) or without this training ("non-experts": n = 45) assessed video clips for ocular motor signs of vestibular deficits on either side or of normal vestibular function.
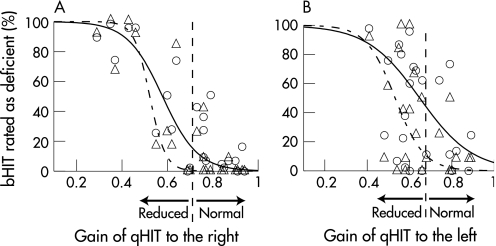
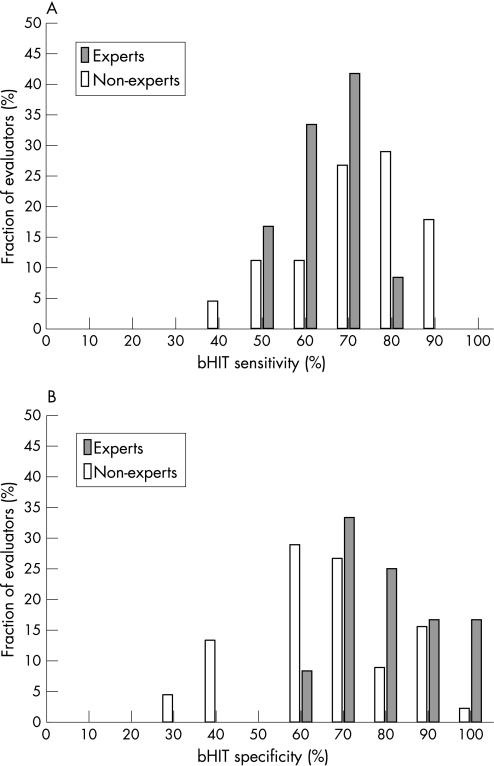
Results: On average, bHIT sensitivity was significantly (t test: p<0.05) lower for experts than for non-experts (63% vs 72%), while bHIT specificity was significantly higher for experts than non-experts (78% vs 64%). This outcome was a consequence of the experts' tendency to accept bHIT with corresponding borderline qHIT values as still being normal. Fitted curves revealed that at the lower normal limit of qHIT, 20% of bHIT were rated as deficient by the experts and 37% by the non-experts.
Conclusions: When qHIT is used as a reference, bHIT sensitivity is adequate and therefore clinically useful in the hands of both neuro-otological experts and non-experts. We advise performing quantitative head impulse testing with search coils or high speed video methods when bHIT is not conclusive.
Conflict of interest statement
Competing interests: None.
References
-
- Halmagyi G M, Curthoys I S. A clinical sign of canal paresis. Arch Neurol 198845737–739. - PubMed
-
- Ewald E J.Physiologische Untersuchungen über das Endorgan des Nervus Octavus. Wiesbaden: Bergmann, 1892
-
- Goldberg J M, Fernandez C. Physiology of peripheral neurons innervating semicircular canals of the squirrel monkey. I. Resting discharge and response to constant angular accelerations. J Neurophysiol 197134635–660. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources