

Treatment of post-transplant premalignant skin disease: a randomized intrapatient comparative study of 5-fluorouracil cream and topical photodynamic therapy
- PMID: 17223873
- PMCID: PMC2423222
- DOI: 10.1111/j.1365-2133.2006.07616.x
Treatment of post-transplant premalignant skin disease: a randomized intrapatient comparative study of 5-fluorouracil cream and topical photodynamic therapy
Abstract
Background: Organ transplant recipients (OTR) are at high risk of developing nonmelanoma skin cancer and premalignant epidermal dysplasia (carcinoma in situ/ Bowen's disease and actinic keratoses). Epidermal dysplasia is often widespread and there are few comparative studies of available treatments.
Objectives: To compare topical methylaminolaevulinate (MAL) photodynamic therapy (PDT) with topical 5% fluorouracil (5-FU) cream in the treatment of post-transplant epidermal dysplasia.
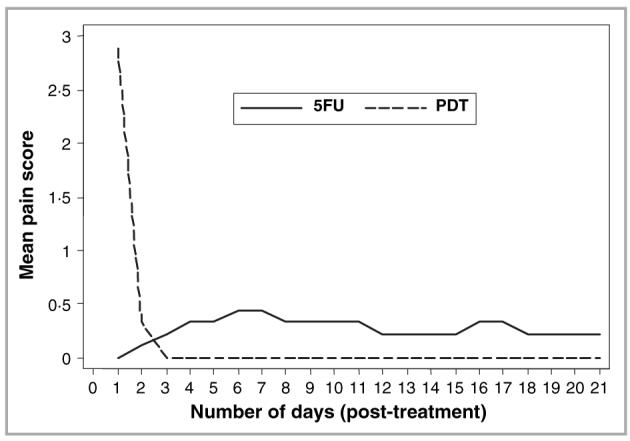
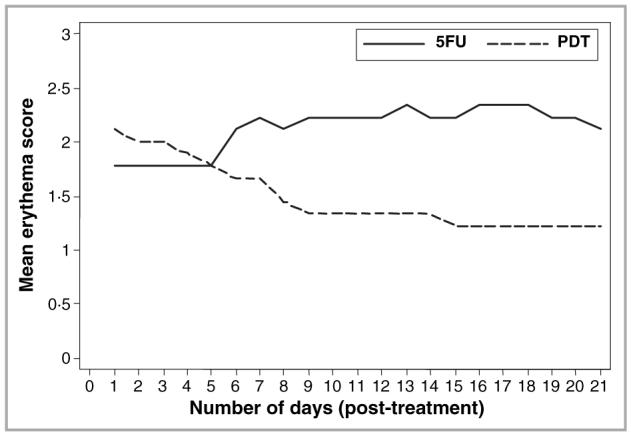
Methods: Eight OTRs with epidermal dysplasia were recruited to an open-label, single-centre, randomized, intrapatient comparative study. Treatment with two cycles of topical MAL PDT 1 week apart was randomly assigned to one area of epidermal dysplasia, and 5-FU cream was applied twice daily for 3 weeks to a clinically and histologically comparable area. Patients were reviewed at 1, 3 and 6 months after treatment. The main outcome measures were complete resolution rate (CRR), overall reduction in lesional area, treatment-associated pain and erythema, cosmetic outcome and global patient preference.
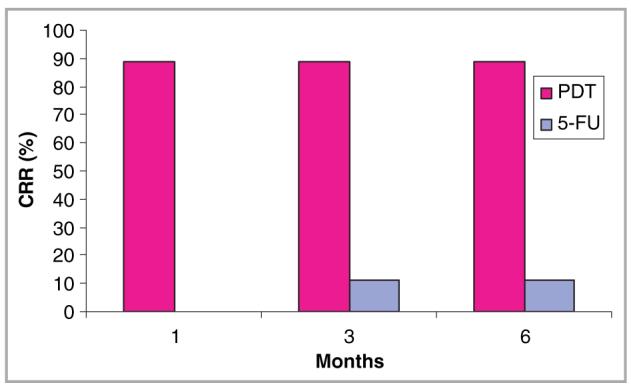
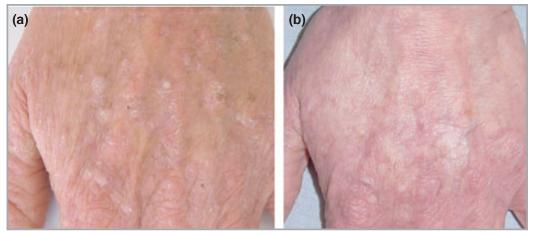
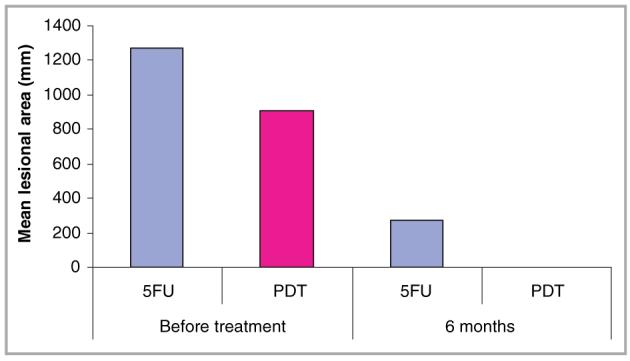
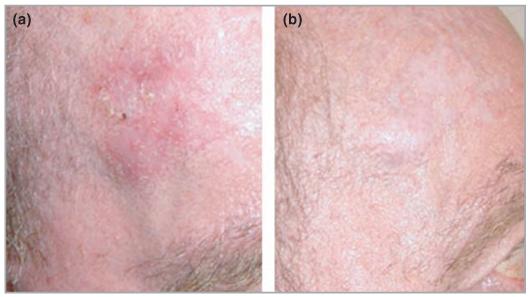
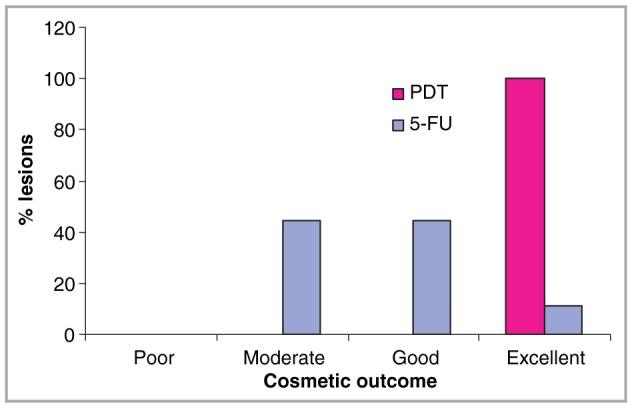
Results: At all time points evaluated after completion of treatment, PDT was more effective than 5-FU in achieving complete resolution: eight of nine lesional areas cleared with PDT (CRR 89%, 95% CI: 0.52-0.99), compared with one of nine lesional areas treated with 5-FU (CRR 11%, 95% CI: 0.003-0.48) (P = 0.02). The mean lesional area reduction was also proportionately greater with PDT than with 5-FU (100% vs. 79% respectively). Cosmetic outcome and patient preference were also superior in the PDT-treated group.
Conclusions: Compared with topical 5-FU, MAL PDT was a more effective and cosmetically acceptable treatment for epidermal dysplasia in OTRs and was preferred by patients. Further studies are now required to confirm these results and to examine the effect of treating epidermal dysplasia with PDT on subsequent development of squamous cell carcinoma in this high risk population.
Figures
References
-
- Penn I. Incidence and treatment of neoplasia after transplantation. J Heart Lung Transplant. 1993;12:S328–36. - PubMed
-
- Euvrard S, Kanitakis J, Claudy A. Skin cancers after organ transplantation. N Engl J Med. 2003;348:1681–91. - PubMed
-
- Jensen P, Hansen S, Moller B, et al. Skin cancer in kidney and heart transplant recipients and different long-term immunosuppressive therapy regimens. J Am Acad Dermatol. 1999;40:177–86. - PubMed
-
- Hartevelt MM, Bavinck JN, Koote AM, et al. Incidence of skin cancer after renal transplantation in The Netherlands. Transplantation. 1990;49:506–9. - PubMed
-
- Ramsay HM, Fryer AA, Hawley CM, et al. Non-melanoma skin cancer risk in the Queensland renal transplant population. Br J Dermatol. 2002;147:950–6. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
