

Skeletal muscle oxygen saturation does not estimate mixed venous oxygen saturation in patients with severe left heart failure and additional severe sepsis or septic shock
- PMID: 17227587
- PMCID: PMC2147710
- DOI: 10.1186/cc5153
Skeletal muscle oxygen saturation does not estimate mixed venous oxygen saturation in patients with severe left heart failure and additional severe sepsis or septic shock
Abstract
Introduction: Low cardiac output states such as left heart failure are characterized by preserved oxygen extraction ratio, which is in contrast to severe sepsis. Near infrared spectroscopy (NIRS) allows noninvasive estimation of skeletal muscle tissue oxygenation (StO2). The aim of the study was to determine the relationship between StO2 and mixed venous oxygen saturation (SvO2) in patients with severe left heart failure with or without additional severe sepsis or septic shock.
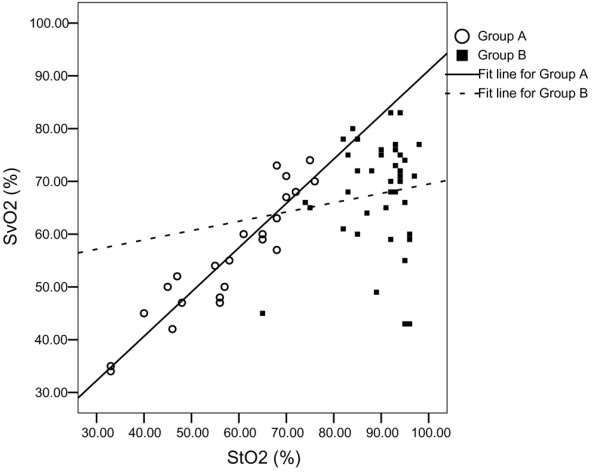
Methods: Sixty-five patients with severe left heart failure due to primary heart disease were divided into two groups: groups A (n = 24) and B (n = 41) included patients without and with additional severe sepsis/septic shock, respectively. Thenar muscle StO2 was measured using NIRS in the patients and in 15 healthy volunteers.
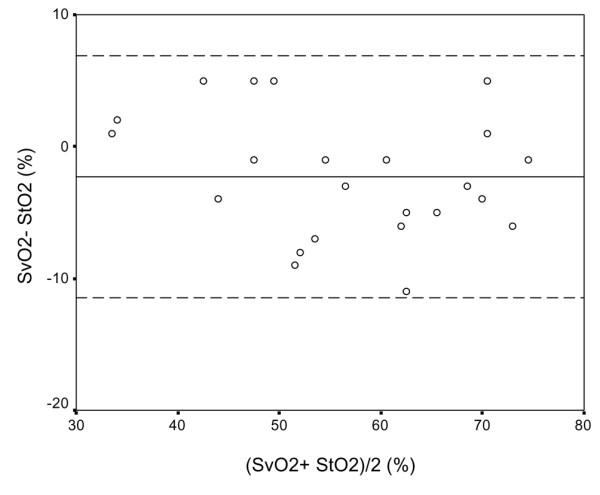
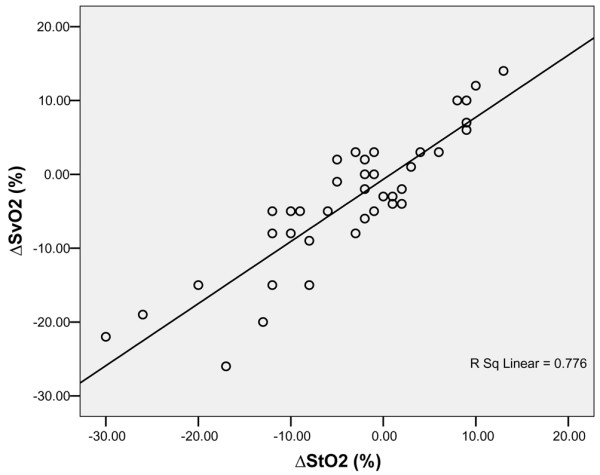
Results: StO2 was lower in group A than in group B and in healthy volunteers (58 +/- 13%, 90 +/- 7% and 84 +/- 4%, respectively; P < 0.001). StO2 was higher in group B than in healthy volunteers (P = 0.02). In group A StO2 correlated with SvO2 (r = 0.689, P = 0.002), although StO2 overestimated SvO2 (bias -2.3%, precision 4.6%). In group A changes in StO2 correlated with changes in SvO2 (r = 0.836, P < 0.001; DeltaSvO2 = 0.84 x DeltaStO2 - 0.67). In group B important differences between these variables were observed. Plasma lactate concentrations correlated negatively with StO2 values only in group A (r = -0.522, P = 0.009; lactate = -0.104 x StO2 + 10.25).
Conclusion: Skeletal muscle StO2 does not estimate SvO2 in patients with severe left heart failure and additional severe sepsis or septic shock. However, in patients with severe left heart failure without additional severe sepsis or septic shock, StO2 values could be used to provide rapid, noninvasive estimation of SvO2; furthermore, the trend in StO2 may be considered a surrogate for the trend in SvO2.
Trial registration: ClinicalTrials.gov NCT00384644.
Figures
Comment in
-
Searching for non-invasive markers of tissue hypoxia.Crit Care. 2007;11(1):116. doi: 10.1186/cc5691. Crit Care. 2007. PMID: 17331268 Free PMC article.
Similar articles
-
Searching for non-invasive markers of tissue hypoxia.Crit Care. 2007;11(1):116. doi: 10.1186/cc5691. Crit Care. 2007. PMID: 17331268 Free PMC article.
-
Near-infrared spectroscopy during stagnant ischemia estimates central venous oxygen saturation and mixed venous oxygen saturation discrepancy in patients with severe left heart failure and additional sepsis/septic shock.Crit Care. 2010;14(2):R42. doi: 10.1186/cc8929. Epub 2010 Mar 23. Crit Care. 2010. PMID: 20331856 Free PMC article. Clinical Trial.
-
The temporal changes of tissue oxygen saturation (StO2) and central venous oxygen saturation (ScvO2) during sepsis/septic shock resuscitation.J Med Assoc Thai. 2014 Mar;97 Suppl 3:S168-75. J Med Assoc Thai. 2014. PMID: 24772595
-
[Factors influencing mixed venous oxygen saturation in intensive care].Ann Fr Anesth Reanim. 1989;8(6):703-7. doi: 10.1016/s0750-7658(89)80195-9. Ann Fr Anesth Reanim. 1989. PMID: 2699177 Review. French.
-
[Venous saturation : Between oxygen delivery and consumption].Med Klin Intensivmed Notfmed. 2017 Sep;112(6):492-498. doi: 10.1007/s00063-016-0145-0. Epub 2016 Mar 1. Med Klin Intensivmed Notfmed. 2017. PMID: 26931134 Review. German.
Cited by
-
Searching for non-invasive markers of tissue hypoxia.Crit Care. 2007;11(1):116. doi: 10.1186/cc5691. Crit Care. 2007. PMID: 17331268 Free PMC article.
-
Restoring arterial pressure with norepinephrine improves muscle tissue oxygenation assessed by near-infrared spectroscopy in severely hypotensive septic patients.Intensive Care Med. 2010 Nov;36(11):1882-9. doi: 10.1007/s00134-010-2013-3. Epub 2010 Aug 6. Intensive Care Med. 2010. PMID: 20689910
-
Comparison of two devices using near-infrared spectroscopy for the measurement of tissue oxygenation during a vascular occlusion test in healthy volunteers (INVOS® vs. InSpectra™).J Clin Monit Comput. 2015 Apr;29(2):271-8. doi: 10.1007/s10877-014-9595-1. Epub 2014 Jul 9. J Clin Monit Comput. 2015. PMID: 25005912
-
Masseter muscle oxygen saturation is associated with central venous oxygen saturation in patients with severe sepsis.J Clin Monit Comput. 2010 Aug;24(4):289-93. doi: 10.1007/s10877-010-9247-z. Epub 2010 Jul 23. J Clin Monit Comput. 2010. PMID: 20652379
-
Monitoring the microcirculation in the critically ill patient: current methods and future approaches.Intensive Care Med. 2010 Nov;36(11):1813-25. doi: 10.1007/s00134-010-2005-3. Epub 2010 Aug 6. Intensive Care Med. 2010. PMID: 20689916 Review.
References
-
- Goldman RH, Klughaupt M, Metcalf T, Spivak AP, Harrison DC. Measurement of central venous oxygen saturation in patients with myocardial infarction. Circulation. 1968;38:941–946. - PubMed
-
- Krafft P, Steltzer H, Hiesmayr M, Klimscha W, Hammerle AF. Mixed venous oxygen saturation in critically ill septic shock patients. The role of defined events. Chest. 1993;103:900–906. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
