

Effective post-exposure treatment of Ebola infection
- PMID: 17238284
- PMCID: PMC1779298
- DOI: 10.1371/journal.ppat.0030002
Effective post-exposure treatment of Ebola infection
Abstract
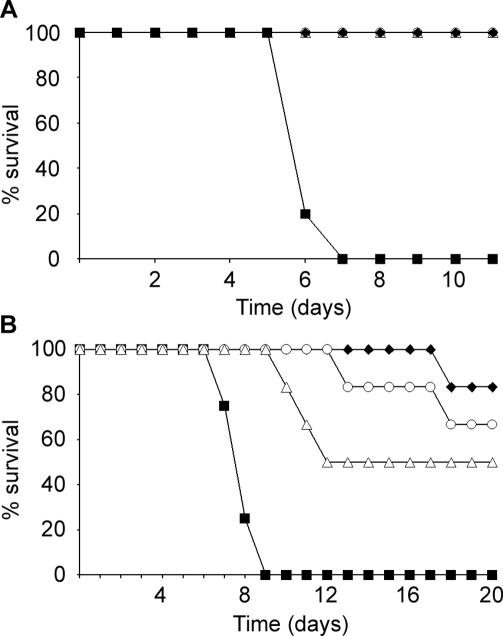
Ebola viruses are highly lethal human pathogens that have received considerable attention in recent years due to an increasing re-emergence in Central Africa and a potential for use as a biological weapon. There is no vaccine or treatment licensed for human use. In the past, however, important advances have been made in developing preventive vaccines that are protective in animal models. In this regard, we showed that a single injection of a live-attenuated recombinant vesicular stomatitis virus vector expressing the Ebola virus glycoprotein completely protected rodents and nonhuman primates from lethal Ebola challenge. In contrast, progress in developing therapeutic interventions against Ebola virus infections has been much slower and there is clearly an urgent need to develop effective post-exposure strategies to respond to future outbreaks and acts of bioterrorism, as well as to treat laboratory exposures. Here we tested the efficacy of the vesicular stomatitis virus-based Ebola vaccine vector in post-exposure treatment in three relevant animal models. In the guinea pig and mouse models it was possible to protect 50% and 100% of the animals, respectively, following treatment as late as 24 h after lethal challenge. More important, four out of eight rhesus macaques were protected if treated 20 to 30 min following an otherwise uniformly lethal infection. Currently, this approach provides the most effective post-exposure treatment strategy for Ebola infections and is particularly suited for use in accidentally exposed individuals and in the control of secondary transmission during naturally occurring outbreaks or deliberate release.
Conflict of interest statement
Figures
References
-
- Feldmann H, Jones S, Klenk HD, Schnittler HJ. Ebola virus: From discovery to vaccine. Nat Rev Immunol. 2003;3:677–685. - PubMed
-
- Geisbert TW, Jahrling PB. Exotic emerging viral diseases: Progress and challenges. Nat Med. 2004;10:110–121. - PubMed
-
- Sanchez A, Khan AS, Zaki SR, Nabel GJ, Ksiazek TG, et al. Filoviridae: Marburg and Ebola viruses. In: Knipe DM, Howley PM, editors. Fields virology. 4th edition. Philadelphia: Lippincott Williams and Wilkins; 2001. pp. 1279–1304.
-
- Walsh PD, Abernethy KA, Bermejo M, Beyers R, De Wachter P, et al. Catastrophic ape decline in western equatorial Africa. Nature. 2003;422:611–614. - PubMed
-
- Feldmann H, Jones SM, Schnittler HJ, Geisbert T. Therapy and prophylaxis of Ebola virus infections. Curr Opin Investig Drugs. 2005;6:823–830. - PubMed
Publication types
MeSH terms
Substances
Associated data
- Actions
- Actions
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
