

Identifying barriers to hypertension guideline adherence using clinician feedback at the point of care
- PMID: 17238390
- PMCID: PMC1839712
Identifying barriers to hypertension guideline adherence using clinician feedback at the point of care
Abstract
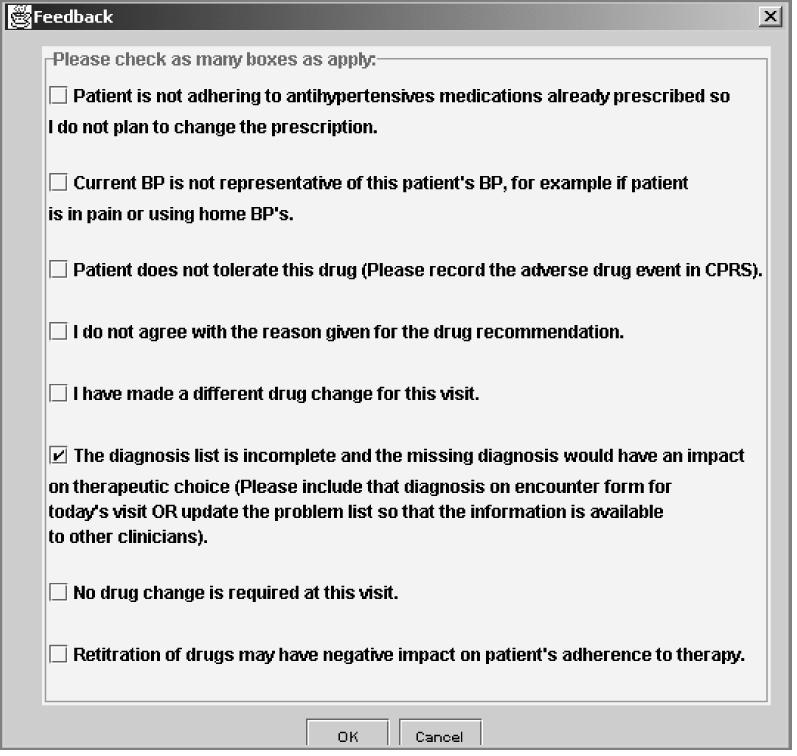
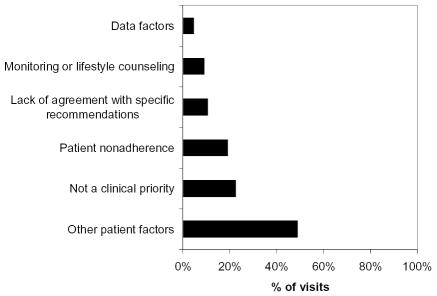
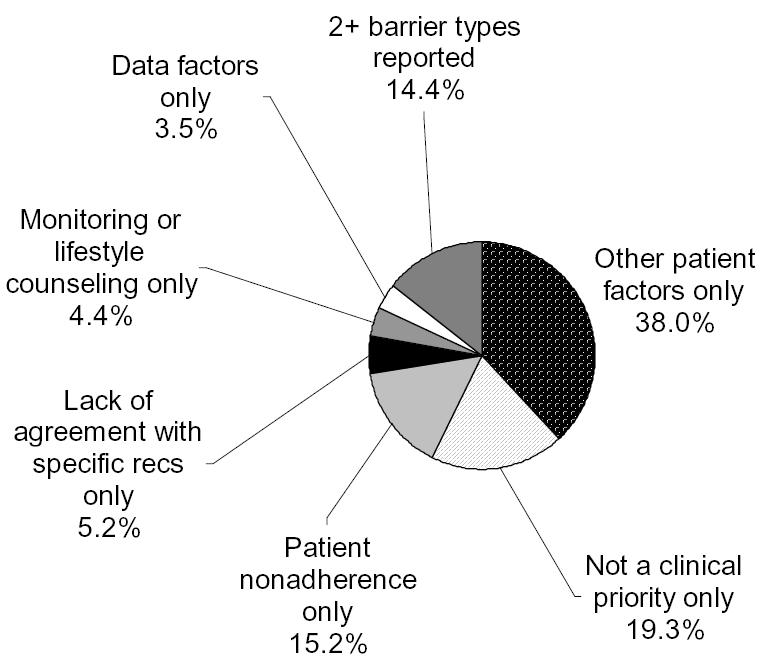
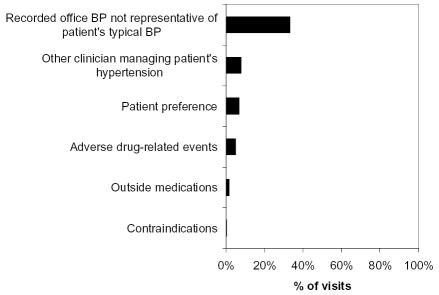
Factors contributing to low adherence to clinical guidelines by clinicians are not well understood. The user interface of ATHENA-HTN, a guideline-based decision support system (DSS) for hypertension, presents a novel opportunity to collect clinician feedback on recommendations displayed at the point of care. We analyzed feedback from 46 clinicians who received ATHENA advisories as part of a 15-month randomized trial to identify potential reasons clinicians may not intensify hypertension therapy when it is recommended. Among the 368 visits for which feedback was provided, clinicians commonly reported they did not follow recommendations because: recorded blood pressure was not representative of the patient's typical blood pressure; hypertension was not a clinical priority for the visit; or patients were nonadherent to medications. For many visits, current quality-assurance algorithms may incorrectly identify clinically appropriate decisions as guideline nonadherent due to incomplete capture of relevant information. We present recommendations for how automated DSSs may help identify "apparent" barriers and better target decision support.
Figures
References
-
- Hajjar I, Kotchen TA. Trends in prevalence, awareness, treatment, and control of hypertension in the United States, 1988–2000. JAMA. 2003;290:199–206. - PubMed
-
- Walsh J, McDonald KM, Shojania KG, et al. Hypertension care. Closing the quality gap: a critical analysis of quality improvement strategies. In: Shojania KG, McDonald KM, et al., editors. Vol. 3. Rockville, MD: AHRQ; 2005. #04-0051-3. - PubMed
-
- Mottur-Pilson C, Snow V, Bartlett K. Physician explanations for failing to comply with "best practices". Eff Clin Pract. 2001;4:207–13. - PubMed
-
- Oliveria SA, Lapuerta P, McCarthy BD, et al. Physician-related barriers to the effective management of uncontrolled hypertension. Arch Intern Med. 2002;162:413–20. - PubMed
-
- Ferrari P, Hess L, Pechere-Bertschi A, Muggli F, Burnier M. Reasons for not intensifying antihypertensive treatment (RIAT): a primary care antihypertensive intervention study. J Hypertens. 2004;22:1221–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical