

New tests of distance stereoacuity and their role in evaluating intermittent exotropia
- PMID: 17241665
- PMCID: PMC2799932
- DOI: 10.1016/j.ophtha.2006.06.066
New tests of distance stereoacuity and their role in evaluating intermittent exotropia
Abstract
Purpose: Poor control of intermittent exotropia has been considered an indication for surgical intervention, and poor distance stereoacuity may be an indicator of poor control. Two new measures of distance stereoacuity, the Frisby-Davis Distance test (FD2) and Distance Randot test (DR), both of which have been validated in normal and strabismic subjects, were evaluated, and we compared stereoacuity with scores on a recently described control scale.
Design: Prospective case series.
Participants: Twenty-five consecutive patients with intermittent exotropia.
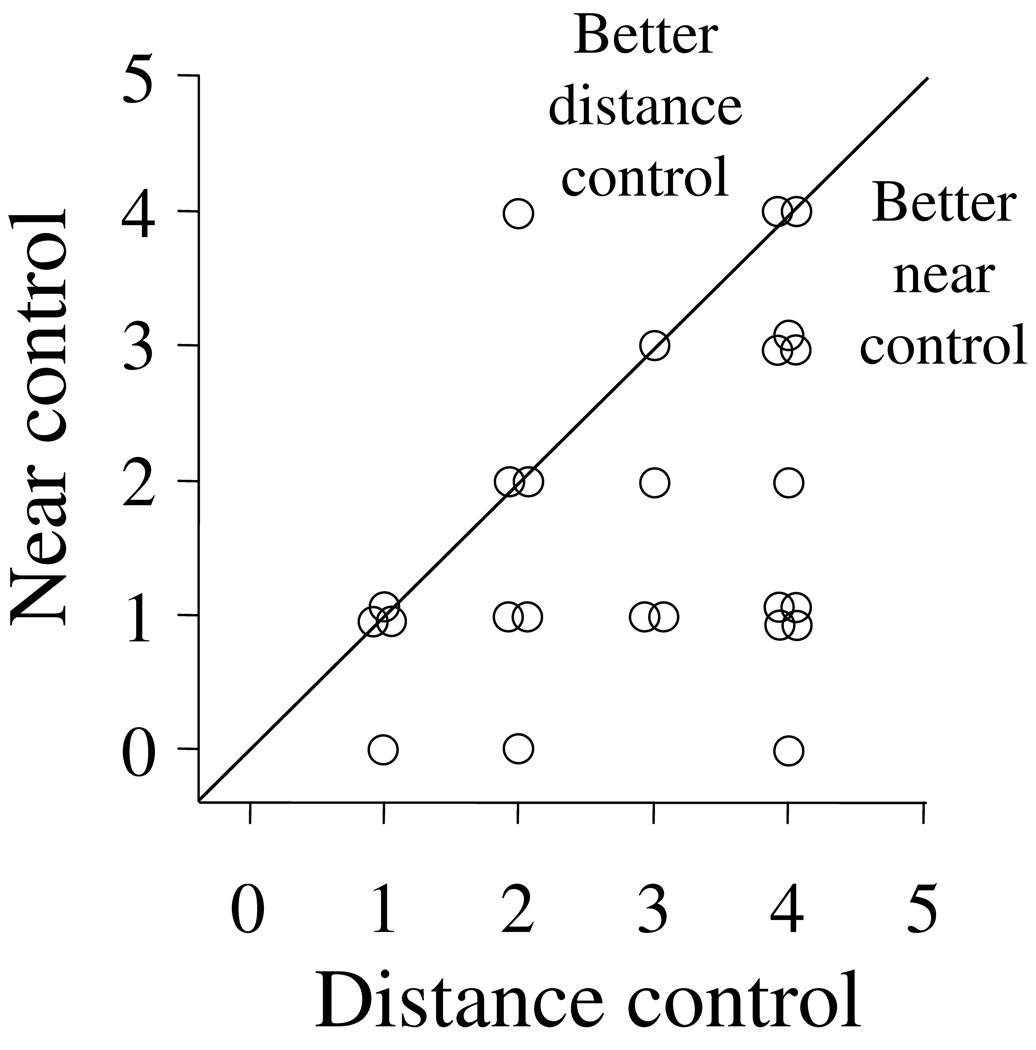
Methods: Office-based control was graded at distance and near on a 0 to 5 scale, and distance control ranged from 1 (recovery in 1-5 seconds after monocular occlusion) to 4 (>50% spontaneously tropic). Stereoacuity was measured using the FD2 and DR at distance and the Preschool Randot and Frisby tests at near.
Main outcome measure: Distance stereoacuity measured using the FD2 and DR.
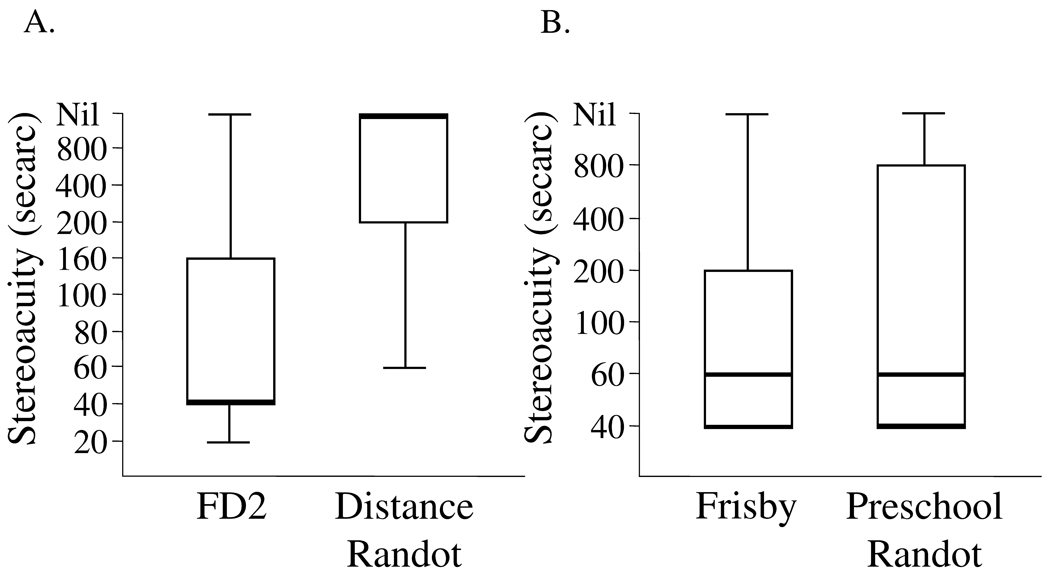
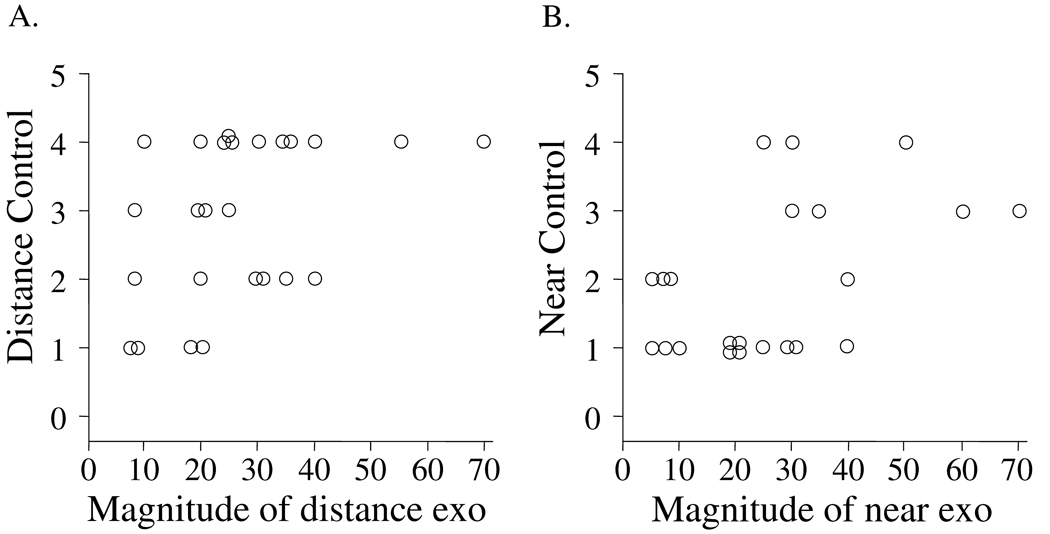
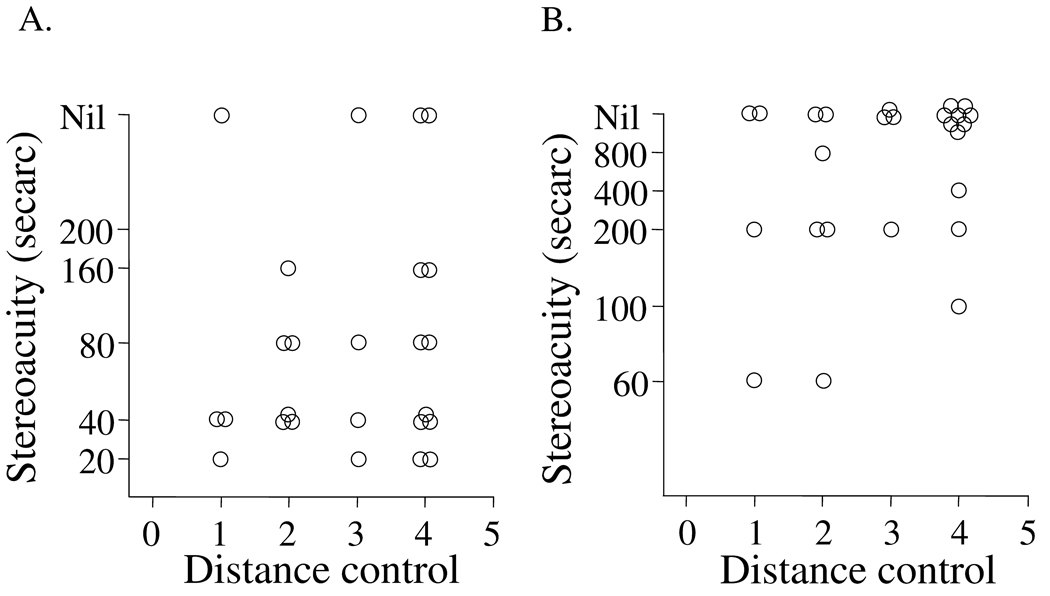
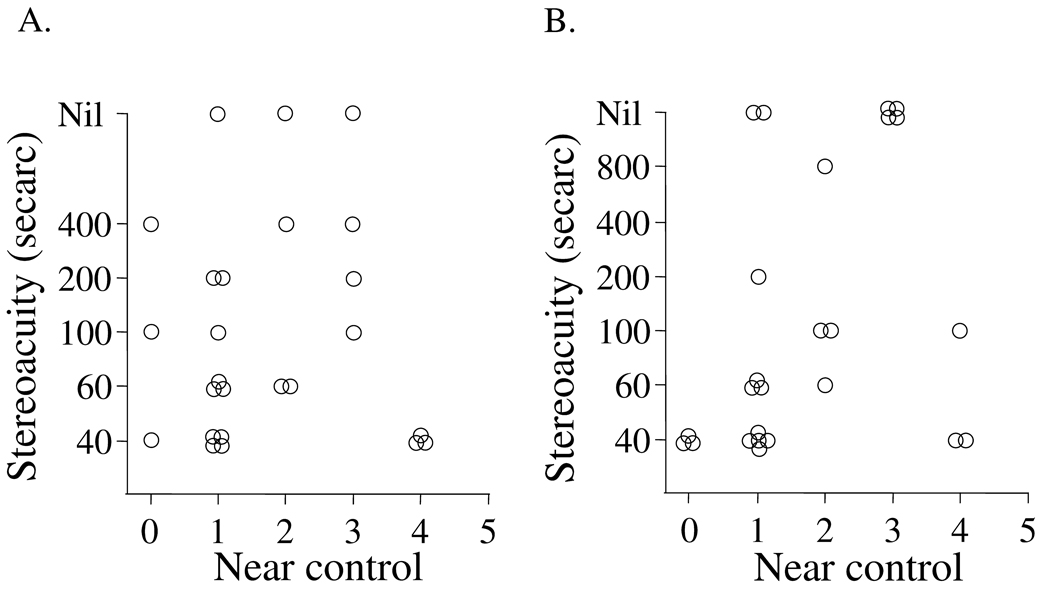
Results: Measurable distance stereoacuity thresholds in intermittent exotropia were poor with the DR and excellent with the FD2 (medians, nil and 40''; P<0.0001). Near stereoacuity was excellent with both the Preschool Randot and Frisby (medians, 60'' and 60''; P = 0.99). There was poor correlation between distance control score and either FD2 (r(s) = 0.1, P = 0.6) or DR (r(s) = 0.3, P = 0.2). Control scores correlated with magnitude of deviation at distance (r(s) = 0.5, P = 0.02) and near (r(s) = 0.5, P = 0.01).
Conclusions: The real-world contour-based targets of the new distance FD2 appear to stimulate fusion in intermittent exotropia, even when distance control is poor. In contrast, the new Polaroid vectograph-based DR is very sensitive to disturbances of binocularity. Two new distance stereoacuity tests appear sensitive to opposite ends of the intermittent exotropia spectrum; FD2 performance deteriorates when the patient is constantly tropic, whereas DR performance deteriorates at the earliest stages of intermittency.
Conflict of interest statement
No conflicting relationships exist
Figures
References
-
- Mohney BG, Huffaker RK. Common forms of childhood exotropia. Ophthalmology. 2003;110:2093–2096. - PubMed
-
- Govindan M, Mohney BG, Diehl NN, Burke JP. Incidence and types of childhood exotropia. A population-based study. Ophthalmology. 2005;112:104–108. - PubMed
-
- Gnanaraj L, Richardson SR. Interventions for intermittent distance exotropia: review. Eye. 2005;19:617–621. - PubMed
-
- Rutstein RP, Corliss DA. The clinical course of intermittent exotropia. Optom Vis Sci. 2003;80:644–649. - PubMed
-
- Abroms AD, Mohney BG, Rush DP, et al. Timely surgery in intermittent and constant exotropia for superior sensory outcome. Am J Ophthalmol. 2001;131:111–116. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
