

Comparison of the outcomes between open and minimally invasive esophagectomy
- PMID: 17245176
- PMCID: PMC1876975
- DOI: 10.1097/01.sla.0000225093.58071.c6
Comparison of the outcomes between open and minimally invasive esophagectomy
Abstract
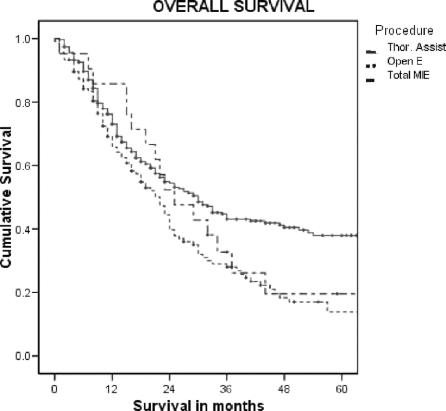
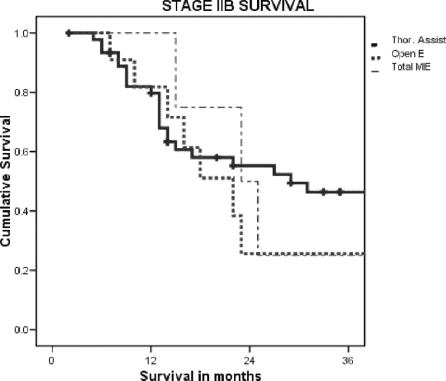
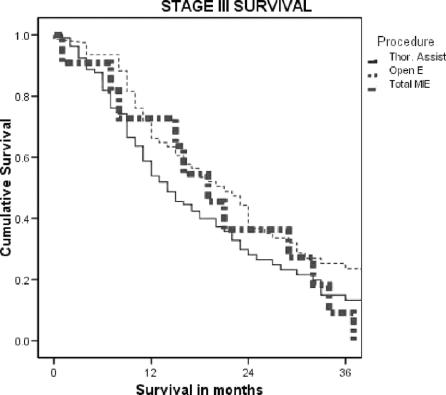
Objective: We report patient outcomes from esophageal resection with respect to morbidity and cancer survival comparing open thoracotomy and laparotomy (Open), with a thoracoscopic/laparotomy approach (Thoracoscopic-Assisted) and a total thoracoscopic/laparoscopic approach (Total MIE).
Methods: From a prospective database of all patients managed with cancer of the esophagus or esophagogastric junction, patients who had a resection using one of three techniques were analyzed to assess postoperative variables, adequacy of cancer clearance, and survival.
Results: The number of patients for each procedure was as follows: Open, 114; Thoracoscopic-Assisted, 309; and Total MIE, 23. The groups were comparable with respect to preoperative variables. The differences in the postoperative variables were: less median blood loss in the Thoracoscopic-Assisted (400 mL) and Total MIE (300 mL) groups versus Open (600 mL); longer time for Total MIE (330 minutes) versus Thoracoscopic-Assisted (285 minutes) and Open (300 minutes); longer median time in hospital for Open (14 days) versus Thoracoscopic-Assisted (13 days), Total MIE (11 days) and less stricture formation in the Open (6.1%) versus Thoracoscopic-Assisted (21.6%), Total MIE (36%). There were no differences in lymph node retrieval for each of the approaches. Open had more stage III patients (65.8%) versus Thoracoscopic-Assisted (34.4%), Total MIE (52.1%). There was no difference in survival when the groups were compared stage for stage for overall median or 3-year survival.
Conclusion: Minimally invasive techniques to resect the esophagus in patients with cancer were confirmed to be safe and comparable to an open approach with respect to postoperative recovery and cancer survival.
Figures
Comment in
-
Re: Comparison of the outcomes between open and minimally invasive esophagectomy.Ann Surg. 2008 Feb;247(2):397; author reply 397-8. doi: 10.1097/SLA.0b013e3181640266. Ann Surg. 2008. PMID: 18216559 No abstract available.
References
-
- Rindani R, Martin C, Cox M. Transhiatal versus Ivor-Lewis oesophagectomy: is there a difference? Aust NZ J Surg. 1999;69:187–194. - PubMed
-
- Rente J, Bull D, Harpole D, et al. Transthoracic versus transhiatal esophagectomy: a prospective study of 945 patients. J Thorac Cardiovasc Surg. 2003;125:1114–1120. - PubMed
-
- Hulscher J, Van Sandick J, De Boer A, et al. Extended transthoracic resection compared with limited transhiatal resection for adenocarcinoma of the esophagus. N Engl J Med. 2002;347:1662–1669. - PubMed
-
- Stein H, Siewert J. Improved prognosis of resected esophageal cancer. World J Surg. 2004;28:520–525. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
