

Anastomotic leaks after intestinal anastomosis: it's later than you think
- PMID: 17245179
- PMCID: PMC1876987
- DOI: 10.1097/01.sla.0000225083.27182.85
Anastomotic leaks after intestinal anastomosis: it's later than you think
Abstract
Purpose: Anastomotic leaks are among the most dreaded complications after colorectal surgery. However, problems with definitions and the retrospective nature of previous analyses have been major limitations. We sought to use a prospective database to define the true incidence and presentation of anastomotic leakage after intestinal anastomosis.
Methods: A prospective database of two colorectal surgeons was reviewed over a 10-year period (1995-2004). The incidence of leak by surgical site, timing of diagnosis, method of detection, and treatment was noted. Complications were entered prospectively by a nurse practitioner directly involved in patient care. Standardized criteria for diagnosis were used. A logistic regression model was used to discriminate statistical variation.
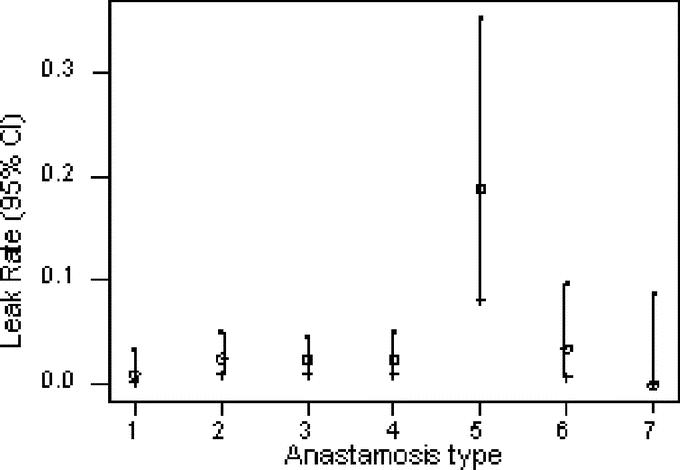
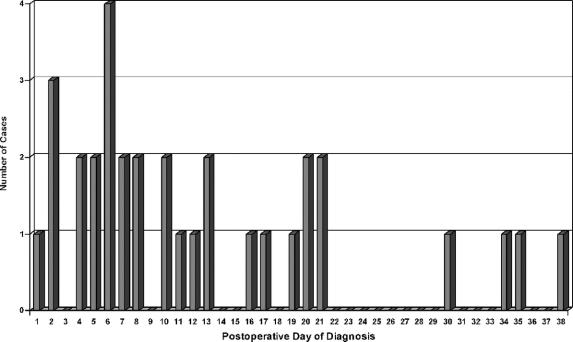
Results: A total of 1223 patients underwent resection and anastomosis during the study period. Mean age was 59.1 years. Leaks occurred in 33 patients (2.7%). Diagnosis was made a mean of 12.7 days postoperatively, including four beyond 30 days (12.1%). There was no difference in leak rate by surgeon (3.6% vs. 2.2%; P = 0.08). The leak rate was similar by surgical site except for a markedly increased leak rate with ileorectal anastomosis (P = 0.001). Twelve leaks were diagnosed clinically versus 21 radiographically. Contrast enema correctly identified only 4 of 10 leaks, whereas CT correctly identified 17 of 19. A total of 14 of 33 (42%) patients had their leak diagnosed only after readmission. Fifteen patients required fecal diversion, whereas 18 could be managed nonoperatively.
Conclusions: Anastomotic leaks are frequently diagnosed late in the postoperative period and often after initial hospital discharge, highlighting the importance of prospective data entry and adequate follow-up. CT scan is the preferred diagnostic modality when imaging is required. More than half of leaks can be managed without fecal diversion.
Figures
References
-
- Golub R, Golub RW, Cantu R, et al. A multivariate analysis of factors contributing to leakage of intestinal anastomosis. J Am Coll Surg. 1997;184:364–372. - PubMed
-
- Detry RJ, Karteuser A, Delriviere L, et al. Use of the circular stapler in 1000 consecutive colorectal anastomoses: experience of one surgical team. Surgery. 1995;117:140–145. - PubMed
-
- Mileski WJ, Joehl RJ, Rege RV, et al. Treatment of anastomotic leakage following low anterior colon resection. Arch Surg. 1988;123:968–971. - PubMed
-
- Hansen O, Schwenk W, Hucke HP, et al. Colorectal stapled anastomoses: experiences and results. Dis Colon Rectum. 1996;39:30–36. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
