

Transcondylar traction as a closed reduction technique in vertically unstable pelvic ring disruption
- PMID: 17245603
- PMCID: PMC2219929
- DOI: 10.1007/s00264-006-0283-8
Transcondylar traction as a closed reduction technique in vertically unstable pelvic ring disruption
Abstract
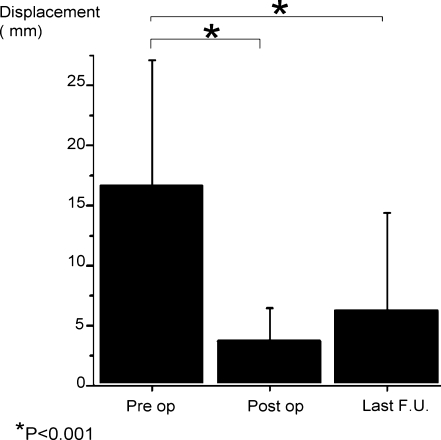
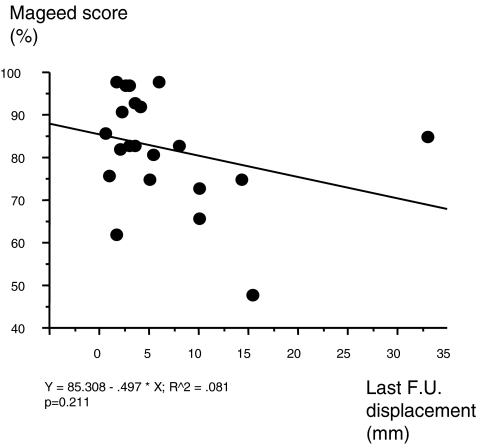
Little information is provided in the literature describing an efficient reduction technique for pelvic ring disruption. The aim of this study is to assess the use of the transcondylar traction as a closed reduction technique for vertically unstable fracture-dislocations of the sacro-iliac joint. Twenty-four pelvic ring disruptions were treated with attempted closed reduction followed by percutaneous screw fixation. Transcondylar traction was used as a closed reduction technique. Closed reduction to within 1 cm of residual displacement was obtained in all cases. No incidence of infection, digestive, cutaneous, or vascular complications occurred. We observed secondary displacement in three patients. Correction of the vertical displacement is better achieved when performed within 8 days after the trauma. Two posterior screws and a complementary anterior fixation is typically required to avoid further displacement in case of sacral fractures. However, an open approach should be preferred in both cases of crescent iliac fracture-sacroiliac dislocation and transforaminal fracture associated with peripheral neurological deficit. A vertical sacral fracture should make the surgeon more wary of fixation failure and loss of reduction.
Introduction: peu d’informations sont données dans la littérature sur les techniques de réduction des ruptures de l’anneau pelvien. Le but de cette étude est d’évaluer l’utilisation d’une traction transfémorale pour les fractures-luxations instables de l’articulation sacro-illiaque. Matériel et méthode: 24 ruptures de l’anneau pelvien ont été réduites par traction transcondylienne puis synthésées par vissage percutanée. Résultat : une réduction a été obtenue avec un déplacement résiduel maximal de 1 cm dans tous les cas. Il n’y a pas eu de problème d’infection, de complication digestive, cutanée ou vasculaire. Nous avons observé trois déplacements secondaires. Discussion: la correction des fractures luxation verticales donne un meilleur résultat si elle est réalisée avant huit jours. Deux vis postérieure et une fixation antérieure complémentaire sont typiquement nécessaires pour éviter des déplacements secondaires, dans les cas de fractures sacré. Cependant un abord chirurgical peut être préféré dans certains cast associant une disjonction sacro iliaque associée à une fracture iliaque ou en cas de fracture sacrée transforaminale associée à des troubles neurologiques. Une fracture sacrée verticale est à haut risque d’échec de fixation et de perte de réduction.
Figures



References
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1097/00005131-199604000-00004', 'is_inner': False, 'url': 'https://doi.org/10.1097/00005131-199604000-00004'}, {'type': 'PubMed', 'value': '8667108', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/8667108/'}]}
- Borrelli J Jr, Koval KJ, Helfet DL (1996) The crescent fracture: a posterior fracture dislocation of the sacroiliac joint. J Orthop Trauma 10(3):165–170 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1097/00005131-200307000-00001', 'is_inner': False, 'url': 'https://doi.org/10.1097/00005131-200307000-00001'}, {'type': 'PubMed', 'value': '12843722', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/12843722/'}]}
- Griffin DR, Starr AJ, Reinert CM, Jones AL, Whitlock S (2003) Vertically unstable pelvic fractures fixed with percutaneous iliosacral screws: does posterior injury pattern predict fixation failure? J Orthop Trauma 17(6):399–405 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1097/00005131-198903010-00008', 'is_inner': False, 'url': 'https://doi.org/10.1097/00005131-198903010-00008'}, {'type': 'PubMed', 'value': '2523480', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/2523480/'}]}
- Henderson RC (1989) The long-term results of nonoperatively treated major pelvic disruptions. J Orthop Trauma 3(1):41–47 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '5084298', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/5084298/'}]}
- Huittinen VM, Slatis P (1972) Fractures of the pelvis. Trauma mechanism, types of injury and principles of treatment. Acta Chir Scand 138:563–569 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '6211739', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/6211739/'}]}
- Letournel E (1981) Surgical fixation of displaced pelvic fractures and dislocations of the symphysis pubis (excluding acetabular fractures). Rev Chir Orthop 67:771–782 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
