

Anorectal and gastric peripheral T-cell lymphoma, unspecified in a non-AIDS patient
- PMID: 17249511
- PMCID: PMC3891034
- DOI: 10.3904/kjim.2006.21.4.262
Anorectal and gastric peripheral T-cell lymphoma, unspecified in a non-AIDS patient
Abstract
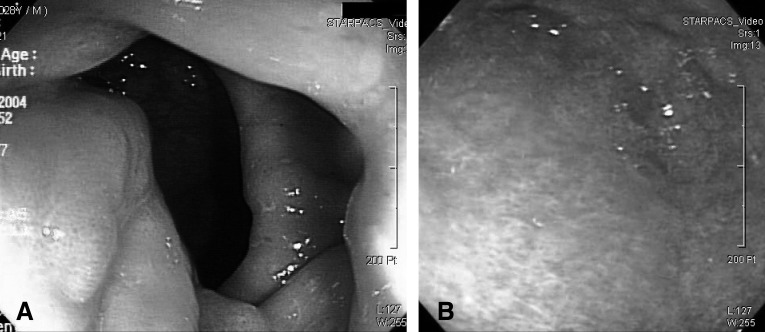
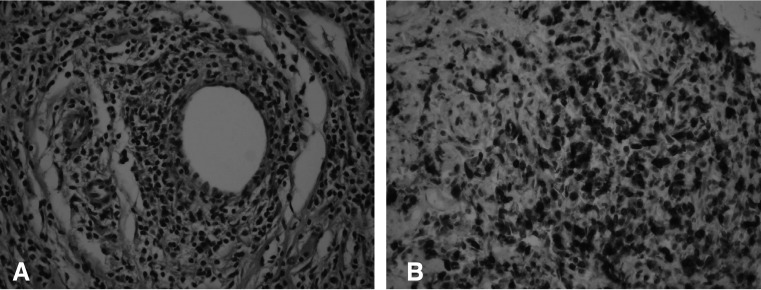
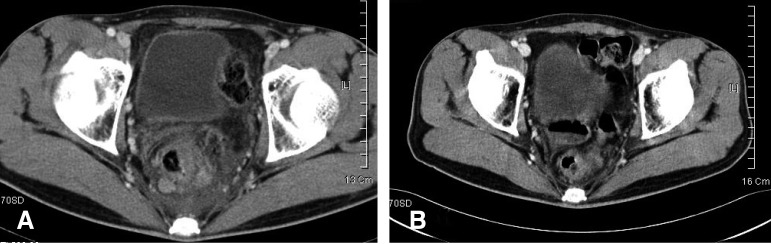
Anorectum is a rare location for malignant lymphoma. Involvement of is rare even for the lynphoma associated with acquired immune deficiency syndrome (AIDS), and AIDS has a relatively increased frequency of anorectal lymphoma. Most lymphomas in AIDS patients are of a B-cell origin, and T-cell lymphoma of the gastrointestinal tract is extremely rare. We report here on a case of anorectal and gastric peripheral T-cell lymphoma, unspecified (PTCLu) in a non-AIDS patient. A previously healthy 29-year-old man presented with hematochezia and tenesmus that he had suffered with for the previous 2 months. Sigmoidoscopy showed anal and rectal submucosal tumor. Multiple round-shaped, flat and elevated lesions were noted on the gastric antrum and body as well. He underwent excisional biopsy for the anal mass and the diagnosis was PTCLu. Biopsies of the gastric lesions gave the same diagnosis. There was no lymphoma involved in the bone marrow. At admission, no antibodies against human immunodeficiency virus were detected. He underwent systemic chemotherapy and upfront autologous stem cell transplantation.
Figures
Similar articles
-
Primary anorectal lymphoma. A new manifestation of the acquired immune deficiency syndrome (AIDS).Cancer. 1987 Oct 1;60(7):1449-53. doi: 10.1002/1097-0142(19871001)60:7<1449::aid-cncr2820600707>3.0.co;2-8. Cancer. 1987. PMID: 2957043
-
Human Herpesvirus Type 8-associated Large B-cell Lymphoma: A Nonserous Extracavitary Variant of Primary Effusion Lymphoma in an HIV-infected Man: A Case Report and Review of the Literature.Clin Lymphoma Myeloma Leuk. 2016 Jun;16(6):311-21. doi: 10.1016/j.clml.2016.03.013. Epub 2016 Apr 1. Clin Lymphoma Myeloma Leuk. 2016. PMID: 27234438 Free PMC article. Review.
-
[Kaposi's sarcoma located in the upper digestive tract. Apropos a case].Rev Esp Enferm Dig. 1991 Nov;80(5):331-4. Rev Esp Enferm Dig. 1991. PMID: 1768473 Spanish.
-
[Non-Hodgkin's lymphoma with perianal localization in patients with acquired immunodeficiency syndrome: a case report].Ann Ital Chir. 1996 Mar-Apr;67(2):277-80. Ann Ital Chir. 1996. PMID: 8929046 Italian.
-
Primary gastric T-cell lymphoma not associated with human T-lymphotropic virus type I: a case report and review of the literature.Ann Hematol. 2003 Mar;82(3):197-202. doi: 10.1007/s00277-003-0612-6. Epub 2003 Feb 13. Ann Hematol. 2003. PMID: 12634958 Review.
References
-
- Aozasa K, Tsujimoto M, Inoue A, Nakagawa K, Hanai J, Kurata A, Nosaka J. Primary gastrointestinal lymphoma: a clinicopathologic study of 102 patients. Oncology. 1985;42:97–103. - PubMed
-
- Place RJ, Huber PJ, Simmang CL. Anorectal lymphoma and AIDS: an outcome analysis. J Surg Oncol. 2000;73:1–4. - PubMed
-
- Ioachim HL, Weinstein MA, Robbins RD, Sohn N, Lugo PN. Primary anorectal lymphoma: a new manifestation of the acquired immune deficiency syndrome (AIDS) Cancer. 1987;60:1449–1453. - PubMed
-
- Ko YH, Kim CW, Park CS, Jang HK, Lee SS, Kim SH, Ree HJ, Lee JD, Kim SW, Huh JR. REAL classification of malignant lymphomas in the Republic of Korea: incidence of recently recognized entities and changes in clinicopathologic features. Cancer. 1998;83:806–812. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical