

Increased alveolar nitric oxide concentration and high levels of leukotriene B(4) and 8-isoprostane in exhaled breath condensate in patients with asbestosis
- PMID: 17251310
- PMCID: PMC2117239
- DOI: 10.1136/thx.2006.067868
Increased alveolar nitric oxide concentration and high levels of leukotriene B(4) and 8-isoprostane in exhaled breath condensate in patients with asbestosis
Abstract
Background: Inhaled asbestos fibres can cause inflammation and fibrosis in the lungs called asbestosis. However, there are no non-invasive means to assess and follow the severity of the inflammation. Exhaled nitric oxide (NO) measured at multiple exhalation flow rates can be used to assess the alveolar NO concentration and bronchial NO flux, which reflect inflammation in the lung parenchyma and airways, respectively. The aim of the present study was to investigate whether exhaled NO or markers in exhaled breath condensate could be used to assess inflammation in asbestosis.
Methods: Exhaled NO and inflammatory markers (leukotriene B(4) and 8-isoprostane) in exhaled breath condensate were measured in 15 non-smoking patients with asbestosis and in 15 healthy controls. Exhaled NO concentrations were measured at four constant exhalation flow rates (50, 100, 200 and 300 ml/s) and alveolar NO concentration and bronchial NO flux were calculated according to the linear model of pulmonary NO dynamics.
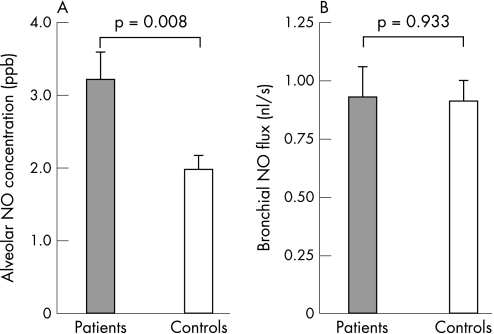
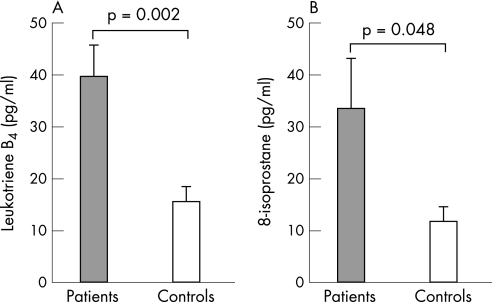
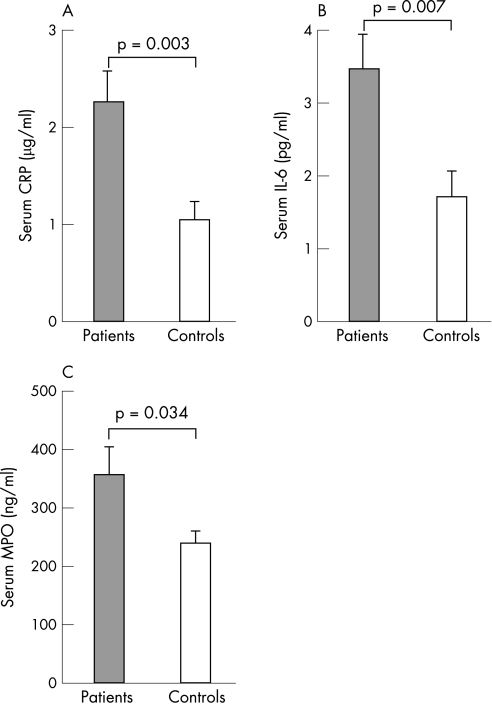
Results: The mean (SE) alveolar NO concentration was significantly higher in patients with asbestosis than in controls (3.2 (0.4) vs 2.0 (0.2) ppb, p = 0.008). There was no difference in bronchial NO flux (0.9 (0.1) vs 0.9 (0.1) nl/s, p = 0.93) or NO concentration measured at ATS standard flow rate of 50 ml/s (20.0 (2.0) vs 19.7 (1.8) ppb, p = 0.89). Patients with asbestosis had increased levels of leukotriene B4 (39.5 (6.0) vs 15.4 (2.9) pg/ml, p = 0.002) and 8-isoprostane (33.5 (9.6) vs 11.9 (2.8) pg/ml, p = 0.048) in exhaled breath condensate and raised serum levels of C-reactive protein (2.3 (0.3) vs 1.1 (0.2) mug/ml, p = 0.003), interleukin-6 (3.5 (0.5) vs 1.7 (0.4) pg/ml, p = 0.007) and myeloperoxidase (356 (48) vs 240 (20) ng/ml, p = 0.034) compared with healthy controls.
Conclusions: Patients with asbestosis have an increased alveolar NO concentration and high levels of leukotriene B4 and 8-isoprostane in exhaled breath. Measurement of exhaled NO at multiple exhalation flow rates and analysis of inflammatory markers in exhaled breath condensate are promising non-invasive means for assessing inflammation in patients with asbestosis.
Conflict of interest statement
Competing interests: None declared.
Similar articles
-
Increased bronchial NO output in severe atopic eczema in children and adolescents.Pediatr Allergy Immunol. 2008 Aug;19(5):426-32. doi: 10.1111/j.1399-3038.2007.00672.x. Epub 2007 Dec 27. Pediatr Allergy Immunol. 2008. PMID: 18167156
-
Leukotriene B4 and 8-isoprostane in exhaled breath condensate of children with episodic and persistent asthma.J Investig Allergol Clin Immunol. 2010;20(3):237-43. J Investig Allergol Clin Immunol. 2010. PMID: 20635789
-
Inflammatory response to sputum induction measured by exhaled markers.Respiration. 2005 Nov-Dec;72(6):594-9. doi: 10.1159/000086721. Epub 2005 Jul 1. Respiration. 2005. PMID: 15988171
-
Exhaled breath condensate: determination of non-volatile compounds and their potential for clinical diagnosis and monitoring. A review.Anal Chim Acta. 2013 Dec 17;805:1-18. doi: 10.1016/j.aca.2013.07.049. Epub 2013 Jul 31. Anal Chim Acta. 2013. PMID: 24296139 Review.
-
Reference Ranges of 8-Isoprostane Concentrations in Exhaled Breath Condensate (EBC): A Systematic Review and Meta-Analysis.Int J Mol Sci. 2020 May 28;21(11):3822. doi: 10.3390/ijms21113822. Int J Mol Sci. 2020. PMID: 32481492 Free PMC article.
Cited by
-
Short-term exposure to stone minerals used in asphalt affect lung function and promote pulmonary inflammation among healthy adults.Scand J Work Environ Health. 2022 Jul 1;48(5):410-418. doi: 10.5271/sjweh.4023. Epub 2022 Mar 21. Scand J Work Environ Health. 2022. PMID: 35312016 Free PMC article. Clinical Trial.
-
Levels of Exhaled Breath Condensate pH and Fractional Exhaled Nitric Oxide in Retired Coal Miners.Toxicol Res. 2010 Dec;26(4):329-37. doi: 10.5487/TR.2010.26.4.329. Toxicol Res. 2010. PMID: 24278541 Free PMC article.
-
Glycoprotein YKL-40 Levels in Plasma Are Associated with Fibrotic Changes on HRCT in Asbestos-Exposed Subjects.Mediators Inflamm. 2017;2017:1797512. doi: 10.1155/2017/1797512. Epub 2017 May 14. Mediators Inflamm. 2017. PMID: 28588347 Free PMC article.
-
Partitioned exhaled nitric oxide to non-invasively assess asthma.Respir Physiol Neurobiol. 2008 Nov 30;163(1-3):166-77. doi: 10.1016/j.resp.2008.07.020. Epub 2008 Jul 31. Respir Physiol Neurobiol. 2008. PMID: 18718562 Free PMC article. Review.
-
Extended Exhaled Nitric Oxide Analysis in Interstitial Lung Diseases: A Systematic Review.Int J Mol Sci. 2020 Aug 27;21(17):6187. doi: 10.3390/ijms21176187. Int J Mol Sci. 2020. PMID: 32867116 Free PMC article.
References
-
- Manning C B, Vallyathan V, Mossman B T. Diseases caused by asbestos: mechanisms of injury and disease development. Int Immunopharmacol 20022191–200. - PubMed
-
- Ross M H, Murray J. Occupational respiratory disease in mining. Occup Med 200454304–310. - PubMed
-
- Bolton C, Richards A, Ebden P. Asbestos‐related disease. Hosp Med 200263148–151. - PubMed
-
- American Thoracic Society Diagnosis and initial management of nonmalignant diseases related to asbestos. Am J Respir Crit Care Med 2004170691–715. - PubMed
-
- Ross R M. The clinical diagnosis of asbestosis in this century requires more than a chest radiograph. Chest 20031241120–1128. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials