

Factors that affect the flow of patients through triage
- PMID: 17251608
- PMCID: PMC2658212
- DOI: 10.1136/emj.2006.036764
Factors that affect the flow of patients through triage
Abstract
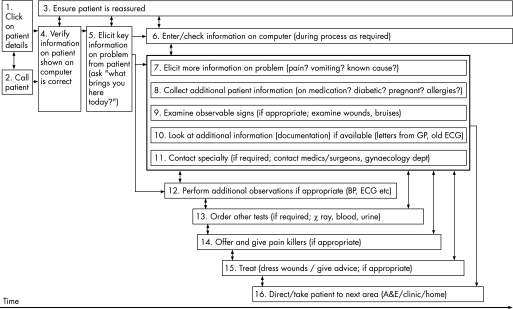
Objective: To use observational methods to objectively evaluate the organisation of triage and what issues may affect the effectiveness of the process.
Design: A two-phase study comprising observation of 16 h of triage in a London hospital emergency department and interviews with the triage staff to build a qualitative task analysis and study protocol for phase 2; observation and timing in triage for 1870 min including 257 patients and for 16 different members of the triage staff.
Results: No significant difference was found between grades of staff for the average triage time or the fraction of time absent from triage. In all, 67% of the time spent absent from triage was due to escorting patients into the department. The average time a patient waited in the reception before triage was 13 min 34 s; the average length of time to triage for a patient was 4 min 17 s. A significant increase in triage time was found when patients were triaged to a specialty, expected by a specialty, or were actively "seen and treated" in triage. Protocols to prioritise patients with potentially serious conditions to the front of the queue had a significantly positive effect on their waiting time. Supplementary tasks and distractions had varying effects on the timely assessment and triage of patients.
Conclusions: The human factors method is applicable to the triage process and can identify key factors that affect the throughput at triage. Referring a patient to a specialty at triage affects significantly the triage workload; hence, alternative methods or management should be suggested. The decision to offer active treatment at triage increases the time taken, and should be based on clinical criteria and the workload determined by staffing levels. The proportion of time absent from triage could be markedly improved by support from porters or other non-qualified staff, as well as by proceduralised handovers from triage to the main clinical area. Triage productivity could be improved by all staff by becoming aware of the effect of the number of interruptions on the throughput of patients.
Conflict of interest statement
Competing interests: None.
References
-
- Department of Health Reforming emergency care: first steps to a new approach. Crown Copyright. London: DOH, 2001
-
- National Health Service Your guide to the NHS. Crown Copyright. London: NHS, 2001
-
- Paulson D L. A comparison of wait times and patients leaving without being seen when licensed nurses versus unlicensed assistive personnel perform triage. J Emerg Nurs. 2004;30: 4, 307–11, - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources