

Treatment of unstable thoracolumbar junction burst fractures with short- or long-segment posterior fixation in magerl type a fractures
- PMID: 17252216
- PMCID: PMC2200786
- DOI: 10.1007/s00586-007-0310-5
Treatment of unstable thoracolumbar junction burst fractures with short- or long-segment posterior fixation in magerl type a fractures
Abstract
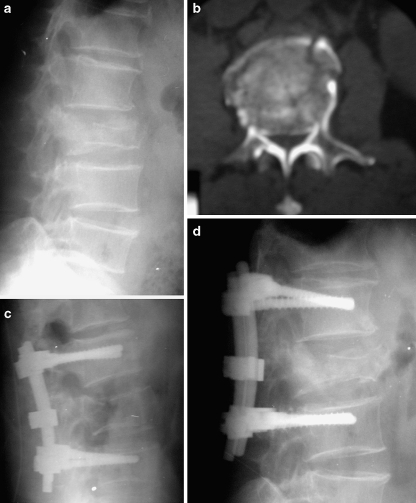
The treatment of thoracolumbar fractures remains controversial. A review of the literature showed that short-segment posterior fixation (SSPF) alone led to a high incidence of implant failure and correction loss. The aim of this retrospective study was to compare the outcomes of the SS- and long-segment posterior fixation (LSPF) in unstable thoracolumbar junction burst fractures (T12-L2) in Magerl Type A fractures. The patients were divided into two groups according to the number of instrumented levels. Group I included 32 patients treated by SSPF (four screws: one level above and below the fracture), and Group II included 31 patients treated by LSPF (eight screws: two levels above and below the fracture). Clinical outcomes and radiological parameters (sagittal index, SI; and canal compromise, CC) were compared according to demographic features, localizations, load-sharing classification (LSC) and Magerl subgroups, statistically. The fractures with more than 10 degrees correction loss at sagittal plane were analyzed in each group. The groups were similar with regard to age, gender, LSC, SI, and CC preoperatively. The mean follow-ups were similar for both groups, 36 and 33 months, respectively. In Group II, the correction values of SI, and CC were more significant than in Group I. More than 10 degrees correction loss occurred in six of the 32 fractures in Group I and in two of the 31 patients in Group II. SSPF was found inadequate in patients with high load sharing scores. Although radiological outcomes (SI and CC remodeling) were better in Group II for all fracture types and localizations, the clinical outcomes (according to Denis functional scores) were similar except Magerl type A33 fractures. We recommend that, especially in patients, who need more mobility, with LSC point 7 or less with Magerl Type A31 and A32 fractures (LSC point 6 or less in Magerl Type A3.3) without neurological deficit, SSPF achieves adequate fixation, without implant failure and correction loss. In Magerl Type A33 fractures with LSC point 7 or more (LSC points 8-9 in Magerl Type A31 and A32) without severe neurologic deficit, LSPF is more beneficial.
Figures

References
-
- Akbarnia BA, Crandall DG, Burkus K, et al. Use of long rods and a short arthrodesis for burst fractures of the thoracolumbar spine. A long-term follow-up study. J Bone Joint Surg Am. 1994;76(11):1629–1635. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
