

Flowcharts for the diagnosis and treatment of acute cholangitis and cholecystitis: Tokyo Guidelines
- PMID: 17252294
- PMCID: PMC2784508
- DOI: 10.1007/s00534-006-1153-x
Flowcharts for the diagnosis and treatment of acute cholangitis and cholecystitis: Tokyo Guidelines
Abstract
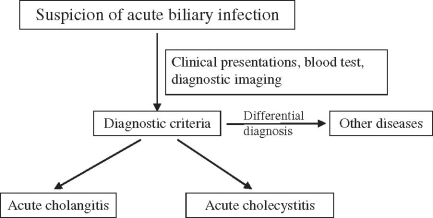
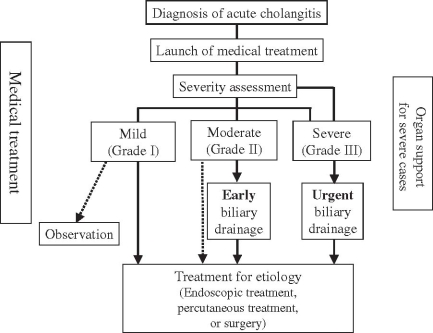
Diagnostic and therapeutic strategies for acute biliary inflammation/infection (acute cholangitis and acute cholecystitis), according to severity grade, have not yet been established in the world. Therefore we formulated flowcharts for the management of acute biliary inflammation/infection in accordance with severity grade. For mild (grade I) acute cholangitis, medical treatment may be sufficient/appropriate. For moderate (grade II) acute cholangitis, early biliary drainage should be performed. For severe (grade III) acute cholangitis, appropriate organ support such as ventilatory/circulatory management is required. After hemodynamic stabilization is achieved, urgent endoscopic or percutaneous transhepatic biliary drainage should be performed. For patients with acute cholangitis of any grade of severity, treatment for the underlying etiology, including endoscopic, percutaneous, or surgical treatment should be performed after the patient's general condition has improved. For patients with mild (grade I) cholecystitis, early laparoscopic cholecystectomy is the preferred treatment. For patients with moderate (grade II) acute cholecystitis, early laparoscopic or open cholecystectomy is preferred. In patients with extensive local inflammation, elective cholecystectomy is recommended after initial management with percutaneous gallbladder drainage and/or cholecystostomy. For the patient with severe (grade III) acute cholecystitis, multiorgan support is a critical part of management. Biliary peritonitis due to perforation of the gallbladder is an indication for urgent cholecystectomy and/or drainage. Delayed elective cholecystectomy may be performed after initial treatment with gallbladder drainage and improvement of the patient's general medical condition.
Figures

References
-
- Lai EC, Mok FP, Tan ES, Lo CM, Fan ST, You KT, et al. Endoscopic biliary drainage for severe acute cholangitis. N Engl J Med. 1992;326:1582–6. - PubMed
-
- Charcot M. De la fievre hepatique symptomatique Comparison avec la fievre uroseptique. Paris: Bourneville et Sevestre; 1877.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
