

Antiretroviral post-exposure prophylaxis (PEP) for occupational HIV exposure
- PMID: 17253483
- PMCID: PMC8989146
- DOI: 10.1002/14651858.CD002835.pub3
Antiretroviral post-exposure prophylaxis (PEP) for occupational HIV exposure
Abstract
Background: Populations such as healthcare workers (HCWs), injection drug users (IDUs), and people engaging in unprotected sex are all at risk of being infected with the human immunodeficiency virus (HIV). Animal models show that after initial exposure, HIV replicates within dendritic cells of the skin and mucosa before spreading through lymphatic vessels and developing into a systemic infection (CDC 2001). This delay in systemic spread leaves a "window of opportunity" for post-exposure prophylaxis (PEP) using antiretroviral drugs designed to block replication of HIV (CDC 2001). PEP aims to inhibit the replication of the initial inoculum of virus and thereby prevent establishment of chronic HIV infection.
Objectives: To evaluate the effects of antiretroviral PEP post-occupational exposure to HIV.
Search strategy: The Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, EMBASE, AIDSearch, and the Database of Abstracts of Reviews of Effectiveness were searched from 1985 to January 2005 to identify controlled trials. There were no language restrictions. Because no controlled clinical trials were retrieved, the search was repeated on 31 May 2005 in MEDLINE, AIDSearch and EMBASE using a search strategy to identify analytic observational studies. Handsearches of the reference lists of all pertinent reviews and studies found were also undertaken. Experts in the field of HIV prevention were contacted.
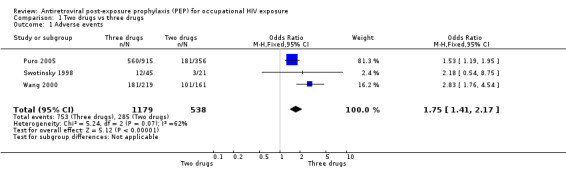
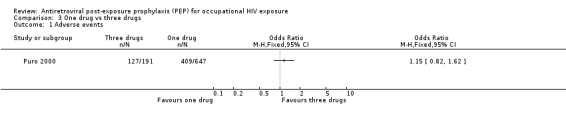
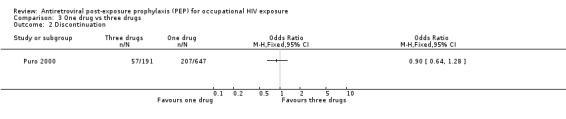
Selection criteria: Types of studies: All controlled trials (including randomized clinical trials and controlled clinical trials). If no controlled trials were found, analytic studies (e.g. cohort and case-control studies) were considered. Descriptive studies (i.e. studies with no comparison groups) were excluded. Types of participants included:HCWs exposed to any known or potentially HIV contaminated product;anyone exposed to a needlestick contaminated by known or potentially HIV-infected blood or other bodily fluid in an occupational setting; andanyone exposed through the mucous membranes to an HIV-infected or potentially infected substance in occupational setting.Excluded: Sex workers (PEP post-sexual exposure is addressed in another Cochrane review (Martín 2005)). Types of interventions: Any intervention that administered single or combinations of antiretrovirals as PEP to people exposed to HIV through percutaneous injuries and/or occupational mucous membrane exposures when the HIV status of the source patient was positive or unknown. Studies comparing two types of PEP regimens were considered, as were studies comparing PEP with no intervention. Types of outcome measures:Incidence of HIV infection in those given PEP versus those given placebo or a different PEP regimen; Adherence to PEP; Complications of PEPTypes of outcome measures: Incidence of HIV infection in those given PEP versus those given placebo or a different PEP regimen; Adherence to PEP; Complications of PEP DATA COLLECTION AND ANALYSIS: Data concerning outcomes, details of the interventions, and other study characteristics were extracted by two independent authors (TY and JA) using a standardized data extraction form (Table 04). A third author (GK) resolved disagreements. The following information was gathered from each included study: location of study, date, publication status, demographics (e.g. age, gender, occupation, risk behavior, etc.) of participants/exposure modality, form of PEP used, duration of use, and outcomes. Odds ratios with a 95% confidence interval (CI) were used as the measure of effect. A meta-analysis was performed for adverse events where two-drug regimens were compared with three-drug regimens. Due to overlap between Puro 2000 and Puro 2005, the former was not included in the combined analysis.
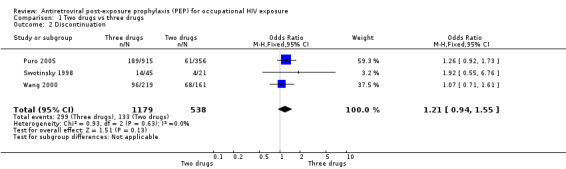
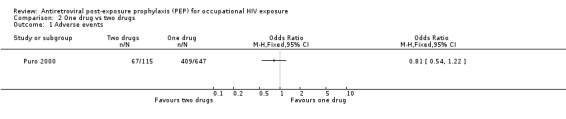
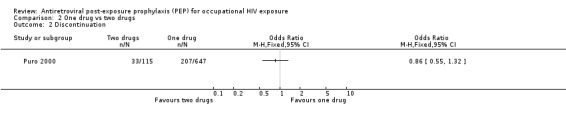
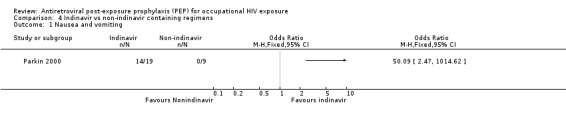
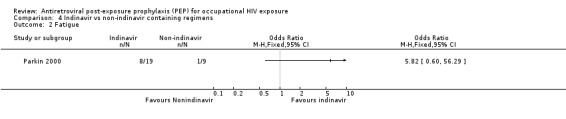
Main results: Effect of PEP on HIV seroconversionNo randomized controlled trials were identified. Only one case-control study was included. HIV transmission was significantly associated with deep injury (OR 15, 95% CI 6.0 to 41), visible blood on the device (OR 6.2, 95% CI 2.2 to 21), procedures involving a needle placed in the source patient's blood vessel (OR 4.3, 95% CI 1.7 to 12), and terminal illness in the source patient (OR 5.6, 95% CI 2.0 to 16). After controlling for these risk factors, no differences were detected in the rates at which cases and controls were offered post-exposure prophylaxis with zidovudine. However, cases had significantly lower odds of having taken zidovudine after exposure compared to controls (OR 0.19, 95%CI 0.06 to 0.52). No studies were found that evaluated the effect of two or more antiretroviral drugs for occupational PEP. Adherence to and complications with PEPEight reports from observational comparative studies confirmed findings that adverse events were higher with a three-drug regimen, especially one containing indinavir. However, discontinuation rates were not significantly different.
Authors' conclusions: The use of occupational PEP is based on limited direct evidence of effect. However, it is highly unlikely that a definitive placebo-controlled trial will ever be conducted, and, therefore, on the basis of results from a single case-control study, a four-week regimen of PEP should be initiated as soon as possible after exposure, depending on the risk of seroconversion. There is no direct evidence to support the use of multi-drug antiretroviral regimens following occupational exposure to HIV. However, due to the success of combination therapies in treating HIV-infected individuals, a combination of antiretroviral drugs should be used for PEP. Healthcare workers should be counseled about expected adverse events and the strategies for managing these. They should also be advised that PEP is not 100% effective in preventing HIV seroconversion. A randomized controlled clinical trial is neither ethical nor practical. Due to the low risk of HIV seroconversion, a very large sample size would be required to have enough power to show an effect. More rigorous evaluation of adverse events, especially in the developing world, are required. Seeing that current practice is partly based on results from individual primary animal studies, we recommend a formal systematic review of all relevant animal studies.
Conflict of interest statement
None known
Figures
Update of
References
References to studies included in this review
Cardo 1997 {published data only}
-
- Cardo DM, Culver DH, Ciesielski CA, et al. A case‐control study of HIV seroconversion in health care workers after percutaneous exposure. NEJM 1997;337(21):1485‐90. - PubMed
ItalianRegistry 2000 {published data only}
-
- Italian Registry of Antiretroviral Post‐exposure Prophylaxis. Effects of short‐course of antiretroviral agents on serum triglycerides of healthy individuals. AIDS 2000;14:2407‐8. - PubMed
Parkin 2000 {published data only}
-
- Parkin JM, Murphy M, Anderson J, et al. Tolerability and side‐effects of post‐exposure prophylaxis for HIV infection. Lancet 2000;355(9205):722‐3. - PubMed
Puro 2000 {published data only}
-
- Puro V for the Italian Registry of Post‐Exposure Prophylaxis. Post‐exposure prophylaxis for HIV infection. Lancet 2000;355:1556‐7. - PubMed
Puro 2003 {published data only}
-
- Puro V, Soldani F, Carli G, Lazarevic Z, Mattioli F, Ippolito G on behalf of the Italian Registry of Antiretroviral Post‐Exposure Prophylaxis. Drug‐induced aminotransferase alterations during antiretroviral HIV post‐exposure prophylaxis. AIDS 2003;17:1988‐90. - PubMed
Puro 2005 {published data only}
-
- Puro V, CArli G, Ippolito G for the Italian Registry of Antiretroviral Post‐Exposure Prophylaxis. Postexposure HIV prophylaxis regimen. Clin Infect Dis 2005;40:205‐6. - PubMed
Srivastava 1998 {published data only}
-
- Srivastava P, Cardo DM, Panlilio A, Campbell S. Tolerability of antiretroviral agents used by health‐care workers (HCWs) as post‐exposure prophylaxis (PEP) for occupational exposures to HIV. Int Conf AIDS, 12:626 (abstract no. 246/33171). 1998.
Swotinsky 1998 {published data only}
-
- Swotinsky RB, Steger KA, Sulis C, Snyder S, Craven DE. Occupational exposure to HIV: experience at a tertiary care center. J Occup and Environ Med 1998;40:1102‐9. - PubMed
Wang 2000 {published data only}
-
- Wang SA, Panlilio AL, Doi PA, White AD, Stek M, Saah A and the HIV PEP Registry Group. Experience of Healthcare Workers Taking Postexposure Prophylaxis after Occupational exposures: findings of the HIV Postexposure Prophylaxis Registry. Infect Control Hosp Epidemiology 2000;21:780‐5. - PubMed
Additional references
Bassett 2004
-
- Bassett IV, Freedberg KA, Walensky RP. Two drugs or three? Balancing efficacy, toxicity, and resistance in postexposure prophylaxis for occupational exposure to HIV. Clin Infect Dis 2004;39:395‐401. - PubMed
Bottinger 1997
-
- Bottinger D, Johansson NG, Samuelsson B, et al. Prevention of simian immunodeficiency virus, SIVsm, or HIV2 infection in cynomolgus monkeys by pre‐ and postexposure administration of BEA‐005. AIDS 1997;11(2):157‐62. - PubMed
Brocklehurst 2002
-
- Brocklehurst P, Volmink J. Antiretrovirals for reducing the risk of mother‐to‐child transmission of HIV infection. The Cochrane Database of Systematic Reviews 2002, Issue 2. - PubMed
CDC 1998b
-
- Center for Disease Control and Prevention. Management of possible sexual, injecting‐drug‐use, or other nonoccupational exposure to HIV, including considerations related to antiretroviral therapy. MMWR 1998;47(RR‐17):1‐18. - PubMed
CDC 2001
-
- Center for Disease Control and Prevention. Updated U.S Public health service guidelines for the management of occupational exposures to HBV, HCV and HIV and recommendations for postexposure prophylaxis. MMWR 2001; Vol. 50, issue RR‐11. - PubMed
CDC 2005
-
- Center for Disease Control and Prevention. Updated U.S. Public health service guidelines for the management of occupational exposures to HIV and recommendations for postexposure prophylaxis. MMWR 2005; Vol. 54, issue RR‐9. - PubMed
Gerberding 2003
-
- Gerberding JL. Occupational exposure to HIV in health care settings. N Engl J Med 2003;348:826‐33. - PubMed
Higgins 2005
-
- Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions 4.2.5 [updated May 2005]. www.cochrane.org/resources/handbook/hbook.htm (accessed 31 May 2005).
Kaldor 2000
-
- Kaldor J. Peer review comments on PEP proposal. e‐mail 2000.
Lee 2001
-
- Lee L, Henderson D. Tolerability of postexposure antiretroviral prophylaxis for occupational exposures to HIV. Drug Safety 2001;24(8):587‐97. - PubMed
Loke 2005
-
- Loke YK, Price D, Herxheimer A on behalf of the Cochrane Adverse Effects Subgroup. Including adverse events. In: Higgins JPT, Green S, editors. www.cochrane.org/resources/handbook/hbook.htm (accessed 31 May 2005).
Low‐Beer 2000
-
- Low‐Beer S, Weber AE, Bartholomew K, et al. A reality check: the cost of making post‐exposure prophylaxis available to gay and bisexual men at high sexual risk. Lancet 2000;14:325‐6. - PubMed
Martín 2005
-
- Martín NV, Almeda J, Casabona J. Effectiveness and safety of HIV post‐exposure prophylaxis after sexual, injecting‐drug‐use or other non‐occupational exposure (Protocol). Cochrane Database of Systematic Reviews 2005, Issue 2.
Miller 1996
-
- Miller S, Lo B, Lurie P, et al. Non‐occupational post‐exposure HIV prophylaxis: guidelines for clinicians. Writing Seminar 1996.
Mori 2000
-
- Mori K, Yasutomi Y, Sawada S, Villinger F, Sugama K, Rosenwith B, et al. Suppression of acute viremia by short‐term postexposure prophylaxis of simian/human immunodeficiency virus SHIV‐RT‐infected monkeys with a novel reverse transcriptase inhibitor (GW420867) allows for development of potent antiviral immune responses resulting in efficient containment of infection. J Virol 2000;74:5747‐53. - PMC - PubMed
Pinkerton 1998
-
- Pinkerton SD, Holtgrave DR, Bloom FR. Cost‐effectiveness of post‐exposure prophylaxis following sexual exposure to HIV. AIDS 1998;12:1067‐1078. - PubMed
Pinkerton 2000
-
- Pinkerton SD, Holtgrave DR, Kahn JG. Is post‐exposure prophylaxis affordable?. AIDS 2000;14:325. - PubMed
Sulkowski 2000
-
- Sulkowski MS, Thomas DL, Chaisson RE, Moore RD. Hepatoxicity associated with antiretroviral therapy in adults infected with human immunodeficiency virus and the role of hepatitis C or B virus infection. JAMA 2000;283:74‐80. - PubMed
Taha 2003
-
- Taha T, Kumwenda N, Gibbons A, Broadhead R, Fiscus S, Lema V, et al. Short postexposure prophylaxis in newborn babies to reduce mother‐to‐child transmission of HIV‐1: NVAZ randomised clinical trial. Lancet 2003;362:1171‐7. - PubMed
Torbati 1999
-
- Torbati SS, Guss DA. Emergency department management of occupational exposures to HIV‐infected fluids. J of Emerg Med 1999;17(2):261‐4. - PubMed
Tsai 1998
-
- Tsai C, Emau P, Follis K, Beck T, Benveniste R, Bischofberger N, et al. Effectiveness of postinoculation (R)‐9‐(2‐phosphonylmethoxypropyl) adenine treatment for prevention of persistent simian immunodeficiency virus SIVmne infection depends critically on timing of initiation and duration of treatment. J Virol 1998;72(4265‐73). - PMC - PubMed
UNAIDS 1998
-
- Laporte A, Aggleton P. HIV/AIDS prevention in the context of new therapies. Report of a meeting organized by UNAIDS and the AIDS Research Institute of the University of California at San Francisco. UNAIDS best practice collection 1998:1‐24.
Wiebe 2000
Yerly 1999
-
- Yerly S, Kaiser L, Race E, Bru J‐P, Clavel F, Perrin L. Transmission of antiretroviral‐drug‐resistent HIV‐1 variants. Lancet 1999;354:729‐33. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous