

Reproducibility of transient elastography in the evaluation of liver fibrosis in patients with chronic liver disease
- PMID: 17255218
- PMCID: PMC1994385
- DOI: 10.1136/gut.2006.111302
Reproducibility of transient elastography in the evaluation of liver fibrosis in patients with chronic liver disease
Abstract
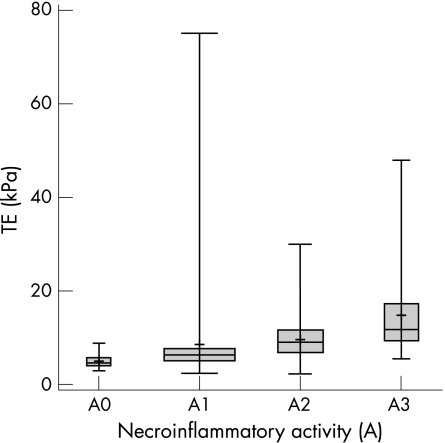
Objective: Transient elastography (TE) is gaining popularity as a non-invasive method for predicting liver fibrosis, but intraobserver and interobserver agreement and factors influencing TE reproducibility have not been adequately assessed. This study investigated these aspects.
Setting: Tertiary referral liver unit.
Patients: Over a 4-month period, 200 patients with chronic liver disease (CLD) with varying aetiology consecutively underwent TE and liver biopsy.
Interventions: TE was performed twice by two different operators either concomitantly or within 3 days of the bioptic procedure (METAVIR classification).
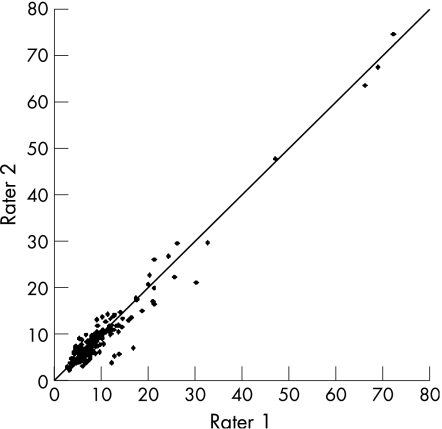
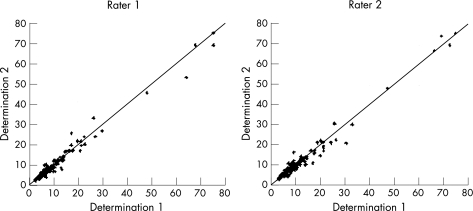
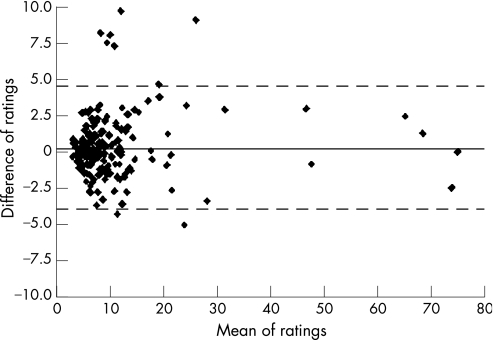
Main outcome measures: Intraobserver and interobserver agreement were analysed using the intraclass correlation coefficient (ICC) and correlated with different patient-related and liver disease-related covariates.
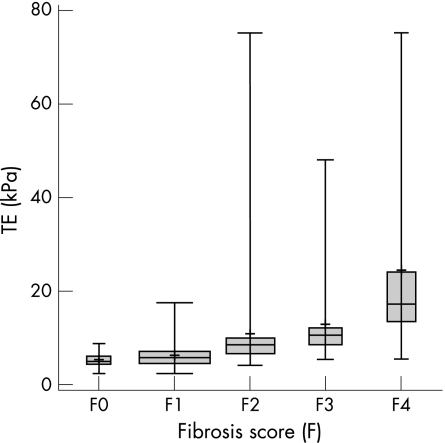
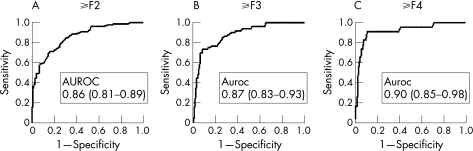
Results: 800 TE examinations were performed, with an indeterminate result rate of 2.4%. The overall interobserver agreement ICC was 0.98 (95% CI 0.977 to 0.987). Increased body mass index (>25 kg/m(2)), steatosis, and low staging grades (fibrosis (F) stage <2) were significantly associated with reduced ICC (p<0.05). Intraobserver agreement ICC was 0.98 for both raters. Using receiver operating characteristic curves, three diagnostic TE thresholds were identified: >7.9 kPa for F>/=2, >10.3 for F>/=3 and >11.9 for F = 4. TE values assessed by the two raters fell within the same cut-off of fibrosis in 88% of the cases for F>/=2, in 92% for F>/=3 and 91% for F = 4.
Conclusions: TE is a highly reproducible and user-friendly technique for assessing liver fibrosis in patients with CLD. However, because TE reproducibility is significantly reduced (p<0.05) in patients with steatosis, increased BMI and lower degrees of hepatic fibrosis, caution is warranted in the clinical use of TE as a surrogate for liver biopsy.
Conflict of interest statement
Competing interests: None to declare
Comment in
-
The non-invasive diagnosis of cirrhosis using the Fibroscan must be performed with cause-specific stiffness cut-offs.Gut. 2008 Nov;57(11):1630; author reply 1630-1. Gut. 2008. PMID: 18941012 No abstract available.
References
-
- Bravo A A, Sheth S G, Chopra S. Liver biopsy.N Engl J Med 2001344495–500. - PubMed
-
- Saadeh S, Cammell G, Carey W D.et al The role of liver biopsy in chronic hepatitis C. Hepatology 200133196–200. - PubMed
-
- Piccinino F, Sagnelli E, Pasquale G.et al Complications following percutaneous liver biopsy. A multicentre retrospective study on 68,276 biopsies. J Hepatol 19862165–173. - PubMed
-
- Bedossa P, Dargere D, Paradis V. Sampling variability of liver fibrosis in chronic hepatitis C. Hepatology 2003381449–1457. - PubMed
-
- Guido M, Rugge M. Liver biopsy sampling in chronic viral hepatitis. Semin Liver Dis 20042489–97. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical