

Labyrinthine lesions and motion sickness susceptibility
- PMID: 17256169
- PMCID: PMC3181155
- DOI: 10.1007/s00221-006-0759-1
Labyrinthine lesions and motion sickness susceptibility
Abstract
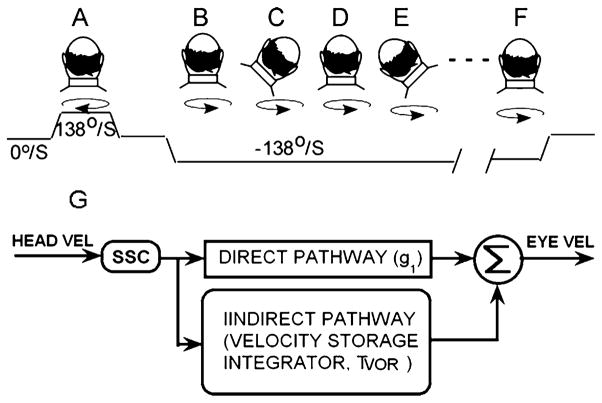
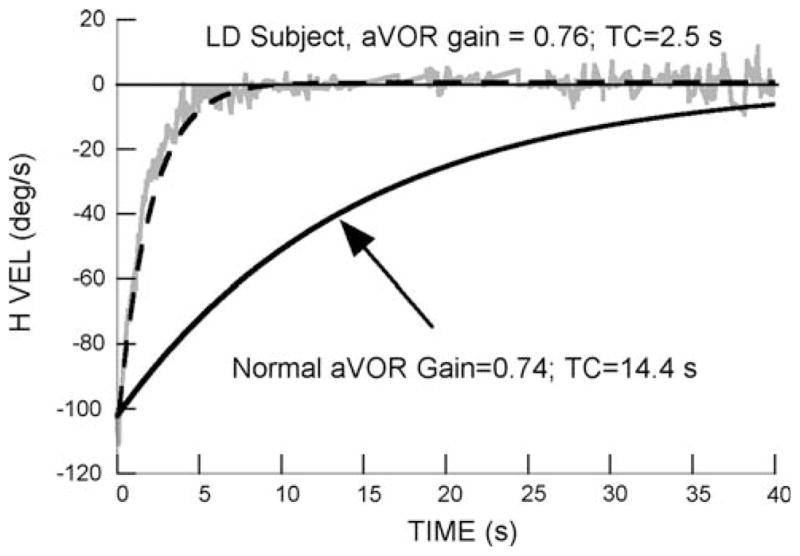
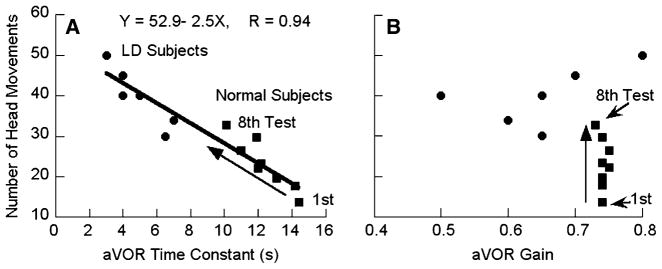
The angular vestibulo-ocular reflex (aVOR) has a fast pathway, which mediates compensatory eye movements, and a slow (velocity storage) pathway, which determines its low frequency characteristics and orients eye velocity toward gravity. We have proposed that motion sickness is generated through velocity storage, when its orientation vector, which lies close to the gravitational vertical, is misaligned with eye velocity during head motion. The duration of the misalignment, determined by the dominant time constant of velocity storage, causes the buildup of motion sickness. To test this hypothesis, we studied bilateral labyrinthine-defective subjects with short vestibular time constants but normal aVOR gains for their motion sickness susceptibility. Time constants and gains were taken from rotational responses. Motion sickness was generated by rolling the head while rotating, and susceptibility was assessed by the number of head movements made before reaching intolerable levels of nausea. More head movements signified lower motion sickness susceptibility. Labyrinthine-defective subjects made more head movements on their first exposure to roll while rotating than normals (39.8 +/- 7.2 vs 13.7 +/- 5.5; P < 0.0001). Normals were tested eight times, which habituated their time constants and reduced their motion sickness susceptibility. Combining data from all subjects, there was a strong inverse relationship between time constants and number of head movements (r = 0.94), but none between motion sickness susceptibility and aVOR gains. This provides further evidence that motion sickness is generated through velocity storage, not the direct pathway, and suggests that motion sickness susceptibility can be reduced by reducing the aVOR time constant.
Figures
References
-
- Balaban CD. Vestibular autonomic regulation (including motion sickness and the mechanism of vomiting) Curr Opin Neurol. 1999;12:29–33. - PubMed
-
- Baloh RW, Hess K, Honrubia V, Yee RD. Low and high frequency sinusoidal rotational testing in patients with vestibular lesions. Acta Otolaryngol Suppl. 1984;406:189–193. - PubMed
-
- Baloh RW, Jacobson K, Honrubia V. Idiopathic bilateral vestibulopathy. Neurology. 1989;39:272–275. - PubMed
-
- Bard P. Subcommittee on motion sickness; Committee on aviation medicine. National Research Council, National Academy of Science; 1945.
-
- Black FO, Gianna-Poulin C, Pesznecker SC. Recovery from vestibular ototoxicity. Otol Neurotol. 2001;22:662–671. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
