

Rapid diagnostic tests compared with malaria microscopy for guiding outpatient treatment of febrile illness in Tanzania: randomised trial
- PMID: 17259188
- PMCID: PMC1804187
- DOI: 10.1136/bmj.39073.496829.AE
Rapid diagnostic tests compared with malaria microscopy for guiding outpatient treatment of febrile illness in Tanzania: randomised trial
Abstract
Objective: To compare rapid diagnostic tests (RDTs) for malaria with routine microscopy in guiding treatment decisions for febrile patients.
Design: Randomised trial.
Setting: Outpatient departments in northeast Tanzania at varying levels of malaria transmission.
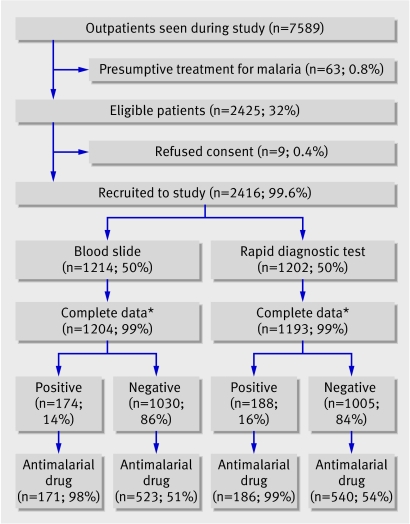
Participants: 2416 patients for whom a malaria test was requested.
Intervention: Staff received training on rapid diagnostic tests; patients sent for malaria tests were randomised to rapid diagnostic test or routine microscopy
Main outcome measure: Proportion of patients with a negative test prescribed an antimalarial drug.
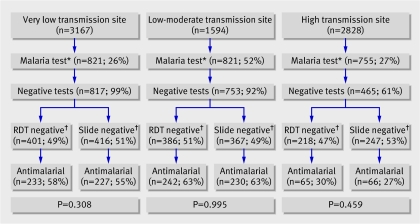
Results: Of 7589 outpatient consultations, 2425 (32%) had a malaria test requested. Of 1204 patients randomised to microscopy, 1030 (86%) tested negative for malaria; 523 (51%) of these were treated with an antimalarial drug. Of 1193 patients randomised to rapid diagnostic test, 1005 (84%) tested negative; 540 (54%) of these were treated for malaria (odds ratio 1.13, 95% confidence interval 0.95 to 1.34; P=0.18). Children aged under 5 with negative rapid diagnostic tests were more likely to be prescribed an antimalarial drug than were those with negative slides (P=0.003). Patients with a negative test by any method were more likely to be prescribed an antibiotic (odds ratio 6.42, 4.72 to 8.75; P<0.001). More than 90% of prescriptions for antimalarial drugs in low-moderate transmission settings were for patients for whom a test requested by a clinician was negative for malaria.
Conclusions: Although many cases of malaria are missed outside the formal sector, within it malaria is massively over-diagnosed. This threatens the sustainability of deployment of artemisinin combination treatment, and treatable bacterial diseases are likely to be missed. Use of rapid diagnostic tests, with basic training for clinical staff, did not in itself lead to any reduction in over-treatment for malaria. Interventions to improve clinicians' management of febrile illness are essential but will not be easy.
Trial registration: Clinical trials NCT00146796 [ClinicalTrials.gov].
Conflict of interest statement
Figures
Comment in
-
Diagnosis and treatment of malaria.BMJ. 2007 Feb 24;334(7590):375-6. doi: 10.1136/bmj.39126.485370.BE. BMJ. 2007. PMID: 17322213 Free PMC article.
-
Stop ambiguous messages on malaria diagnosis.BMJ. 2007 Mar 10;334(7592):489. doi: 10.1136/bmj.39143.024838.1F. BMJ. 2007. PMID: 17347193 Free PMC article. No abstract available.
References
-
- World Health Organization, UNICEF. The Africa malaria report 2003. Geneva: WHO, 2003:70-112. (WHO/CDS/MAL/2003.1093 ed.)
-
- Chandramohan D, Jaffar S, Greenwood B. Use of clinical algorithms for diagnosing malaria. Trop Med Int Health 2002;7:45-52. - PubMed
-
- Kallander K, Nsungwa-Sabiiti J, Peterson S. Symptom overlap for malaria and pneumonia—policy implications for home management strategies. Acta Trop 2004;90:211-4. - PubMed
-
- Amexo M, Tolhurst R, Barnish G, Bates I. Malaria misdiagnosis: effects on the poor and vulnerable. Lancet 2004;364:1896-8. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical