

Progression from newly acquired impaired fasting glusose to type 2 diabetes
- PMID: 17259486
- PMCID: PMC1851903
- DOI: 10.2337/dc06-1392
Progression from newly acquired impaired fasting glusose to type 2 diabetes
Erratum in
- Diabetes Care. 2008 Dec;31(12):2414
Abstract
Objective: We sought to estimate the rate of progression from newly acquired (incident) impaired fasting glucose (IFG) to diabetes under the old and new IFG criteria and to identify predictors of progression to diabetes.
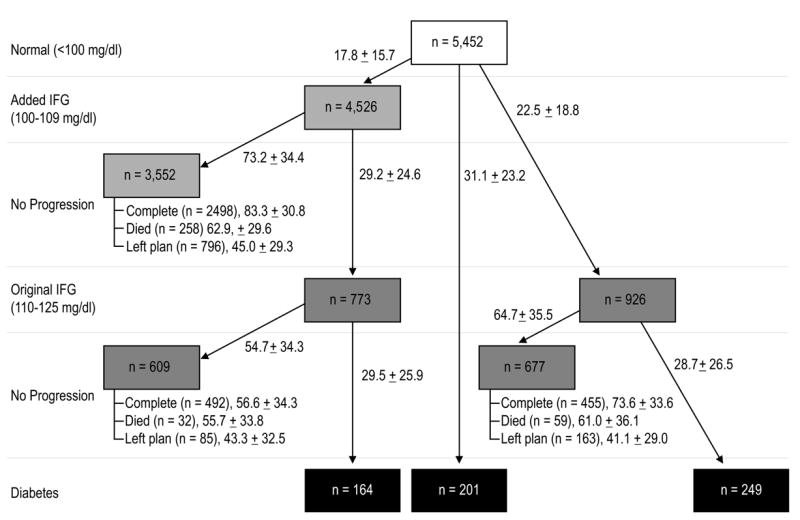
Research design and methods: We identified 5,452 members of an HMO with no prior history of diabetes, with at least two elevated fasting glucose tests (100-125 mg/dl) measured between 1 January 1994 and 31 December 2003, and with a normal fasting glucose test before the two elevated tests. All data were obtained from electronic records of routine clinical care. Subjects were followed until they developed diabetes, died, left the health plan, or until 31 December 2005.
Results: Overall, 8.1% of subjects whose initial abnormal fasting glucose was 100-109 mg/dl (added IFG subjects) and 24.3% of subjects whose initial abnormal fasting glucose was 110-125 mg/dl (original IFG subjects) developed diabetes (P < 0.0001). Added IFG subjects who progressed to diabetes did so within a mean of 41.4 months, a rate of 1.34% per year. Original IFG subjects converted at a rate of 5.56% per year after an average of 29.0 months. A steeper rate of increasing fasting glucose; higher BMI, blood pressure, and triglycerides; and lower HDL cholesterol predicted diabetes development.
Conclusions: To our knowledge, these are the first estimates of diabetes incidence from a clinical care setting when the date of IFG onset is approximately known under the new criterion for IFG. The older criterion was more predictive of diabetes development. Many newly identified IFG patients progress to diabetes in <3 years, which is the currently recommended screening interval.
Figures
Comment in
-
Progression from newly acquired impaired fasting glucose to type 2 diabetes: response to Nichols et al.Diabetes Care. 2007 Jul;30(7):e79; author reply e80. doi: 10.2337/dc07-0530. Diabetes Care. 2007. PMID: 17596502 No abstract available.
References
-
- American Diabetes Association. Standards of medical care for patients with diabetes mellitus; Clinical practice recommendations 2006. Diabetes Care. 2006;29(Supplement 1):S1–S85.
-
- Unwin N, Shaw J, Zimmet P, Alberti KGMM. Impaired glucose tolerance and impaired fasting glycaemia: the current status on definition and intervention. Diabet Med. 2002;19:708–723. - PubMed
-
- de Vegt F, Dekker JM, Jager A, Hienkens E, Kostense PJ, Stehouwer CDA, et al. Relation of impaired fasting and postload glucose with incident type 2 diabetes in a Dutch population. JAMA. 2001;285 (16):2109–2113. - PubMed
-
- Eschwege E, Charles MA, Simon D, Thibult N, Balkau B. Reproducibility of the diagnosis of diabetes over a 30-month follow-up: The Paris Prospective Study. Diabetes Care. 2001;24 (11):1941–1944. - PubMed
-
- Vaccaro O, Ruffa G, Imperatore G, Iovino V, Rivellese AA, Riccardi G. Risk of diabetes in the new diagnostic category of impaired fasting glucose: a prospective analysis. Diabetes Care. 1999;22:1490–1493. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
