

Liver dysfunction after lung recruitment manoeuvres during pressure-controlled ventilation in experimental acute respiratory distress
- PMID: 17261192
- PMCID: PMC2151872
- DOI: 10.1186/cc5674
Liver dysfunction after lung recruitment manoeuvres during pressure-controlled ventilation in experimental acute respiratory distress
Abstract
Introduction: Consequences of lung recruitment with prolonged high positive end-expiratory pressure (PEEP) ventilation for liver function are unclear. We therefore investigated liver dysfunction during two different ventilation treatment regimens of experimental acute respiratory distress syndrome.
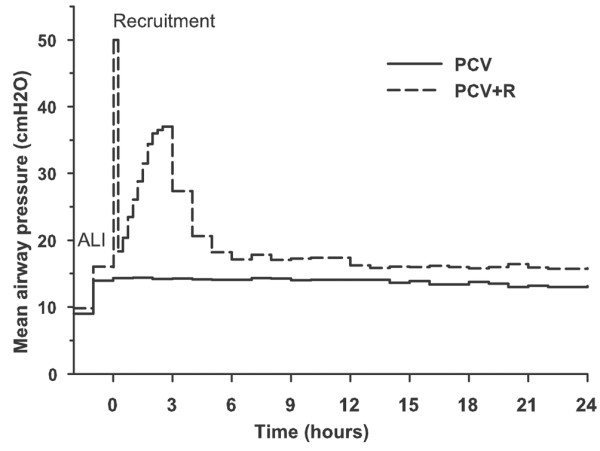
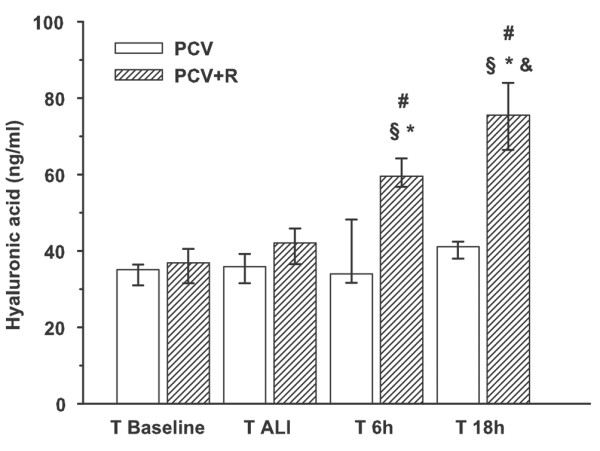
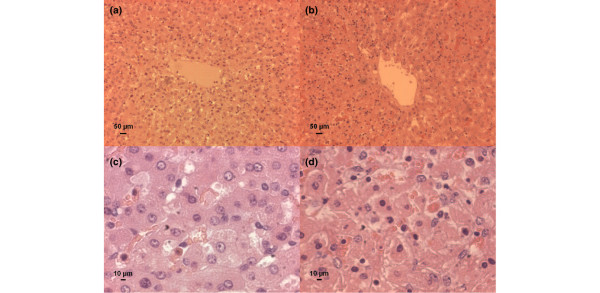
Methods: Sixteen anaesthetised juvenile pietrain pigs were ventilated in the pressure-controlled mode (PCV) with an inspiratory fraction of oxygen (FiO2) of 1.0, a respiratory frequency of 30 per minute, a tidal volume of 6 ml/kg, and a PEEP of 5 cm H2O. After lung injury was induced by repeated pulmonary lavage with normal saline, animals were randomly assigned into two groups (n = 8 each) for a 24-hour trial: PCV (unchanged ventilation) and PCV with recruitment (PCV+R) (starting with a sustained inflation of 50 cm H2O for 1 minute, the ventilation was continued while increasing PEEP in increments of 3 cm H2O every 15 minutes as long as arterial oxygen tension [PaO2] improved). After recruitment, FiO2 was reduced to 0.4 and the PEEP was lowered every 15 minutes until PaO2 decreased to 12.0 to 14.7 kPa (90 to 110 torr). Serum levels of hyaluronic acid (HA), routine liver serum markers, and plasma disappearance rate of indocyanine green (ICG) were tested before and after lung injury, and 6 and 18 hours after randomisation. Liver serum markers were also tested at 24 hours. Paraffin sections of liver tissue stained by haematoxylin and eosin were made after euthanisation.
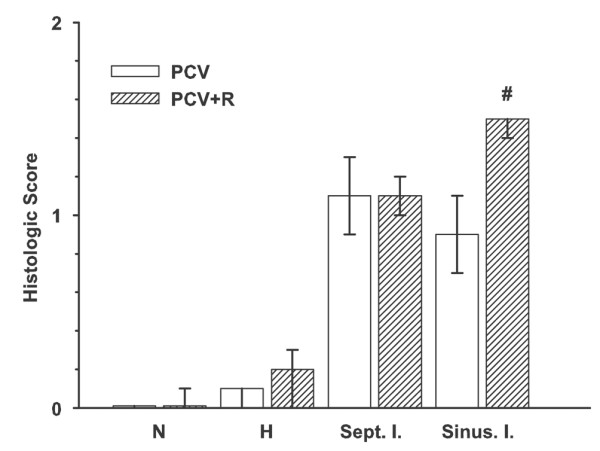
Results: The PCV+R group exhibited more polymorphonuclear neutrophils and lymphocytes in the liver sinusoids: median score (interquartile range) of 1.5 (1.4 to 1.5) compared to 0.9 (0.7 to 1.1) (p = 0.01). Elevation of bilirubin, aspartate aminotransferase, and lactate dehydrogenase was more prominent in the PCV+R group. Plasma disappearance rate of ICG indicated no liver dysfunction. HA levels in the PCV+R group gradually increased and were significantly higher (p < 0.001) at 6 and 18 hours with 59 (57 to 64) and 75 (66 to 84) ng/ml, respectively, than in the PCV group with 34 (32 to 48) and 41 (38 to 42) ng/ml, respectively.
Conclusion: The PCV+R group showed a more prominent inflammatory reaction in their liver sinusoids accompanied by increased serum levels of liver enzymes and HA. Therefore, recruitment with higher PEEP levels for treatment of respiratory failure might lead to liver dysfunction.
Figures
Comment in
-
Myocardial injury associated with hyperinflation of the lung.Crit Care. 2007;11(2):412; author reply 412. doi: 10.1186/cc5738. Crit Care. 2007. PMID: 17466084 Free PMC article. No abstract available.
Similar articles
-
The effect of mode, inspiratory time, and positive end-expiratory pressure on partial liquid ventilation.Am J Respir Crit Care Med. 1999 Apr;159(4 Pt 1):1087-95. doi: 10.1164/ajrccm.159.4.9711021. Am J Respir Crit Care Med. 1999. PMID: 10194150
-
[Positive end-expiratory pressure and tidal volume titration after recruitment maneuver in a canine model of acute respiratory distress syndrome].Zhonghua Jie He He Hu Xi Za Zhi. 2005 Nov;28(11):763-8. Zhonghua Jie He He Hu Xi Za Zhi. 2005. PMID: 16324272 Chinese.
-
Hepatic effects of an open lung strategy and cardiac output restoration in an experimental lung injury.Acta Anaesthesiol Scand. 2010 May;54(5):632-42. doi: 10.1111/j.1399-6576.2009.02192.x. Epub 2010 Jan 6. Acta Anaesthesiol Scand. 2010. PMID: 20055766
-
Lung recruitment maneuvers in acute respiratory distress syndrome and facilitating resolution.Crit Care Med. 2003 Apr;31(4 Suppl):S265-71. doi: 10.1097/01.CCM.0000057902.29449.29. Crit Care Med. 2003. PMID: 12682451 Review.
-
Controversies when using mechanical ventilation in obese patients with and without acute distress respiratory syndrome.Expert Rev Respir Med. 2019 May;13(5):471-479. doi: 10.1080/17476348.2019.1599285. Epub 2019 Apr 5. Expert Rev Respir Med. 2019. PMID: 30919705 Review.
Cited by
-
Hypercapnic hyperventilation shortens emergence time from Propofol and Isoflurane anesthesia.J Res Pharm Pract. 2013 Jan;2(1):24-8. doi: 10.4103/2279-042X.114085. J Res Pharm Pract. 2013. PMID: 24991600 Free PMC article.
-
Acute Lung Injury Regulation by Hyaluronan.J Allergy Ther. 2011 Dec 20;Suppl 4:10.4172/2155-6121.S4-003. doi: 10.4172/2155-6121.S4-003. J Allergy Ther. 2011. PMID: 24244887 Free PMC article.
-
Levobupivacaine plasma concentrations following major liver resection.J Anesth. 2011 Jun;25(3):369-75. doi: 10.1007/s00540-011-1107-6. Epub 2011 Mar 3. J Anesth. 2011. PMID: 21365353 Clinical Trial.
-
[Cholestasis and liver dysfunction in critical care patients].Anaesthesist. 2008 Dec;57(12):1172-82. doi: 10.1007/s00101-008-1459-y. Anaesthesist. 2008. PMID: 18989650 Review. German.
-
Supervised Machine Learning Models for Predicting Sepsis-Associated Liver Injury in Patients With Sepsis: Development and Validation Study Based on a Multicenter Cohort Study.J Med Internet Res. 2025 May 26;27:e66733. doi: 10.2196/66733. J Med Internet Res. 2025. PMID: 40418571 Free PMC article.
References
-
- Imai Y, Parodo J, Kajikawa O, de Perrot M, Fischer S, Edwards V, Cutz E, Liu M, Keshavjee S, Martin TR, et al. Injurious mechanical ventilation and end-organ epithelial cell apoptosis and organ dysfunction in an experimental model of acute respiratory distress syndrome. JAMA. 2003;289:2104–2112. doi: 10.1001/jama.289.16.2104. - DOI - PubMed
-
- Matuschak GM, Pinsky MR, Rogers RM. Effects of positive end-expiratory pressure on hepatic blood flow and performance. J Appl Physiol. 1987;62:1377–1383. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
