

Chronic kidney disease associated mortality in diastolic versus systolic heart failure: a propensity matched study
- PMID: 17261405
- PMCID: PMC2708087
- DOI: 10.1016/j.amjcard.2006.08.042
Chronic kidney disease associated mortality in diastolic versus systolic heart failure: a propensity matched study
Abstract
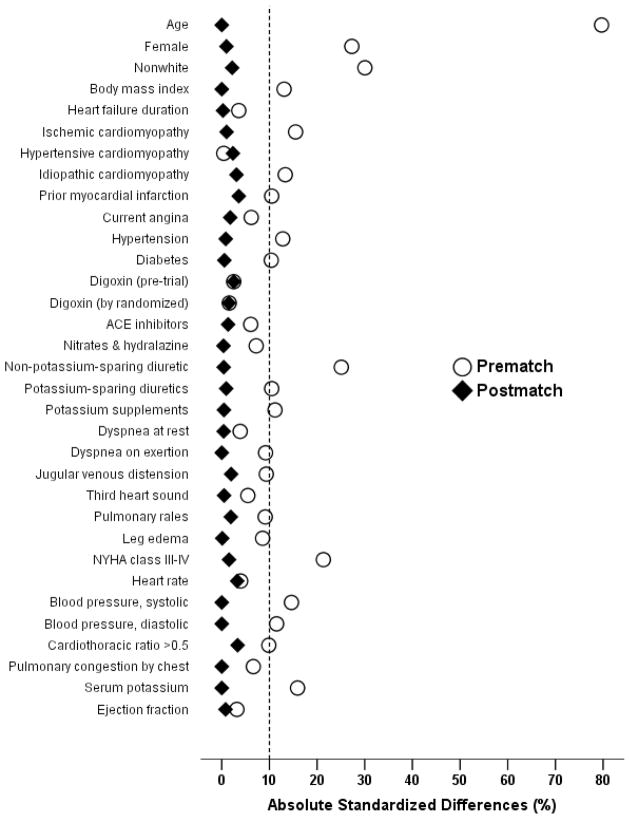
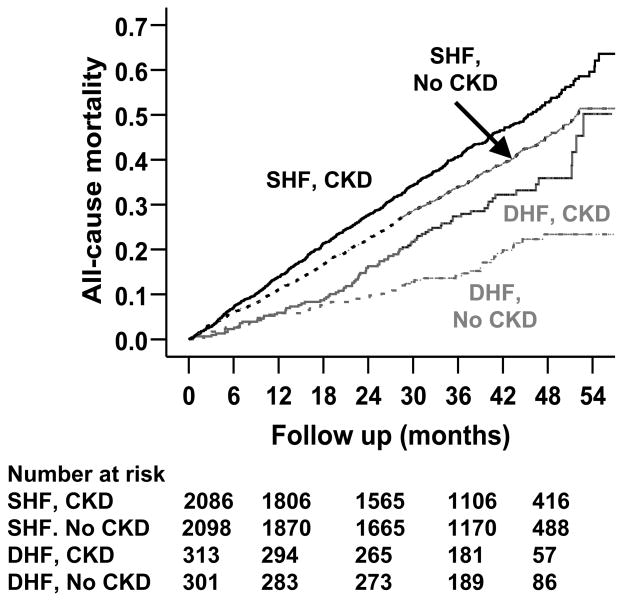
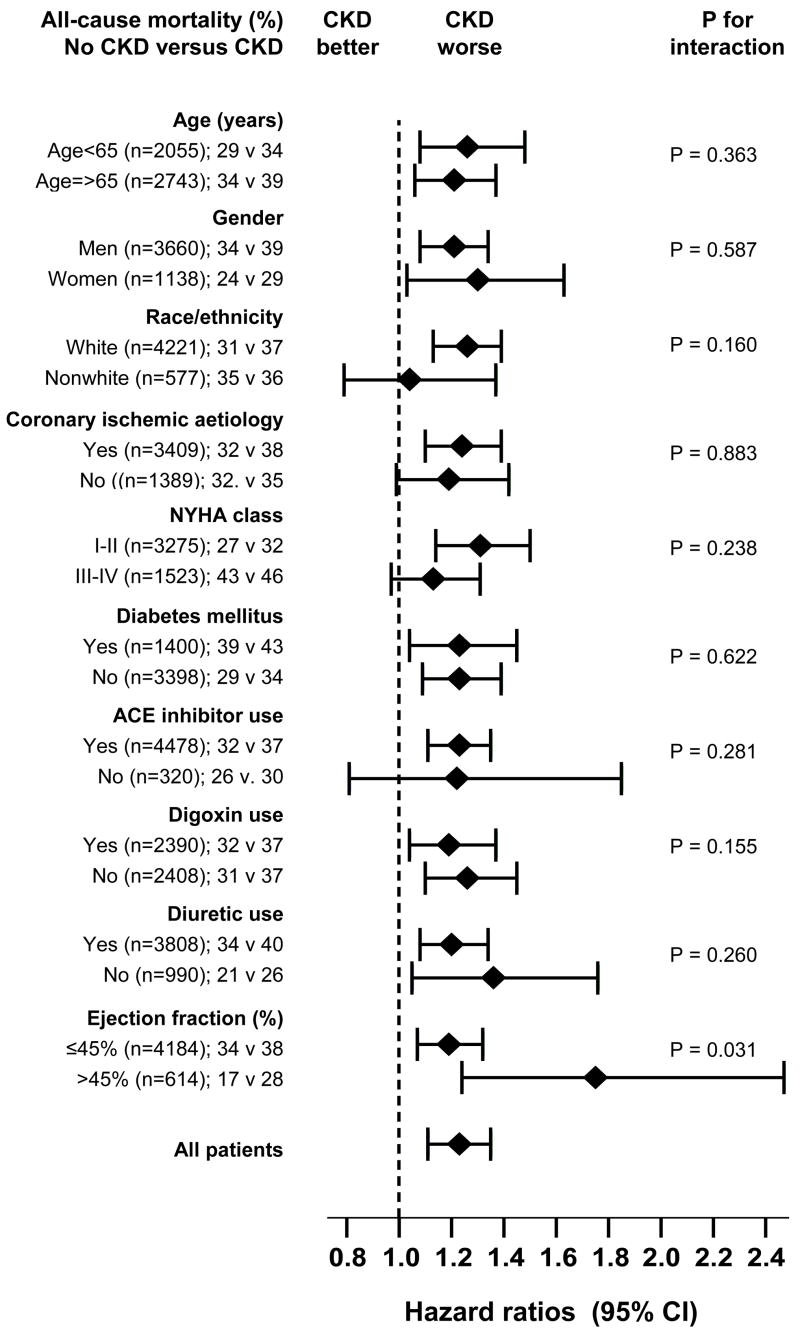
Chronic kidney disease (CKD) is common and is associated with increased mortality in heart failure (HF). However, it is unknown whether the effect of CKD on mortality varies by left ventricular ejection fraction (LVEF). We evaluated the effect of CKD on mortality in patients with systolic (LVEF <or=45%) and diastolic (LVEF >45%) HF. Of the 7,788 patients in the Digitalis Investigation Group trial, 3,527 (45%) had CKD (estimated glomerular filtration rate <60 ml/min/1.73 m2). We calculated the propensity score for CKD for each patient, using a multivariate logistic regression model (c statistic 0.76, postmatch absolute standardized differences <5% for all 32 co-variates). We matched 2,399 pairs of patients with and without CKD with similar propensity scores. There were 757 (rate 1,049/10,000 person-years) and 882 (rate 1,282/10,000 person-years) deaths, respectively, in patients without and with CKD (hazard ratio 1.22, 95% confidence interval 1.09 to 1.36, p <0.0001). CKD-associated mortality was higher in those with diastolic HF (371 extra deaths/10,000 person-years, hazard ratio 1.71, 95% confidence interval 1.21 to 2.41, p = 0.002) than in systolic HF (214 extra deaths/10,000 person-years, hazard ratio 1.19, 95% confidence interval 1.07 to 1.32, p = 0.001), which was significant (adjusted p for interaction = 0.034). A graded association was found between CKD-related deaths and LVEF. The hazard ratios for CKD-associated mortality for the LVEF subgroups of <35%, 35% to 55%, and >55% were 1.15 (95% confidence interval 1.02 to 1.29), 1.35 (95% confidence interval 1.11 to 1.64), and 2.33 (95% confidence interval 1.34 to 4.06). In conclusion, CKD-associated mortality was higher in those with diastolic than systolic HF. Patients with diastolic HF should be evaluated for CKD, and the role of inhibitors of the renin-angiotensin system in these patients needs to be investigated.
Conflict of interest statement
Figures
References
-
- Shlipak MG, Smith GL, Rathore SS, Massie BM, Krumholz HM. Renal function, digoxin therapy, and heart failure outcomes: evidence from the digoxin intervention group trial. J Am Soc Nephrol. 2004;15:2195–2203. - PubMed
-
- Ahmed A, Kiefe CI, Allman RM, Sims RV, DeLong JF. Survival benefits of angiotensin-converting enzyme inhibitors in older heart failure patients with perceived contraindications. J Am Geriatr Soc. 2002;50:1659–1666. - PubMed
-
- McAlister FA, Ezekowitz J, Tonelli M, Armstrong PW. Renal insufficiency and heart failure: prognostic and therapeutic implications from a prospective cohort study. Circulation. 2004;109:1004–1009. - PubMed
-
- Rosenbaum PR, Rubin DB. Reducing bias in observational studies using subclassification on the propensity score. J Am Stat Asso. 1984;79:516–524.
-
- Rubin DB. Using propensity score to help design observational studies: Application to the tobacco litigation. Health Services and Outcomes Research Methodology. 2001;2:169–188.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
