

Mortality and incidence of second cancers following treatment for testicular cancer
- PMID: 17262080
- PMCID: PMC2360021
- DOI: 10.1038/sj.bjc.6603589
Mortality and incidence of second cancers following treatment for testicular cancer
Abstract
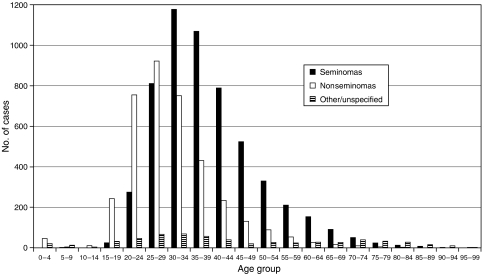
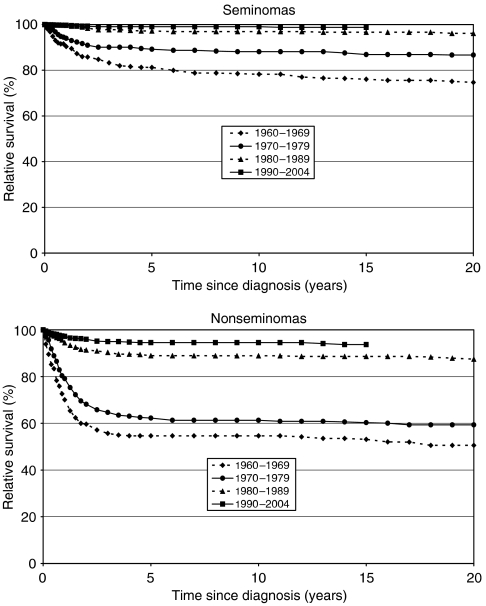
We studied 5555 seminoma patients and 3733 patients with nonseminomatous testicular cancers diagnosed in Southeast England between 1960 and 2004. For both groups survival improved over time: 10-year relative survival increased from 78% in 1960-1969 to 99% in 1990-2004 for seminomas, and from 55 to 95% for nonseminomas. In the early period mortality was still significantly increased more than 15 years after diagnosis in both groups, whereas in more recent periods the excess deaths mainly occurred in the first 5 years after diagnosis. For seminomas, there was a significant excess of cancers of the colon (standardised incidence ratio (SIR) 2.36; 95% confidence interval (CI) 1.13-4.35), soft tissue (SIR 13.64; CI 1.65-49.28) and bladder (SIR 4.28; CI 2.28-7.31) in the long term (20+ years after diagnosis), of pancreatic cancer in both the medium (10-19 years) (SIR 2.91; CI 1.26-5.73) and long term (SIR 5.48; CI 2.37-10.80), of leukaemia in both the short (0-9 years) (SIR 3.01; CI 1.44-5.54) and long term (SIR 4.48; CI 1.64-9.75), and of testis cancer in both the short (SIR 6.69; CI 4.28-9.95) and medium term (SIR 3.96; CI 1.08-10.14). For nonseminomas, significant excesses were found in the long term for cancers of the stomach (SIR 5.13; CI 1.40-13.13), rectum (SIR 4.49; CI 1.22-11.51) and pancreas (SIR 10.17: CI 3.73-22.13), and for testis cancer in the medium term (SIR 5.94; CI 2.18-12.93). Leukaemia was significantly increased in the short term (SIR 6.78; CI 2.93-13.36). The better survival observed is largely attributable to improved treatment, and the trend in reducing the toxicity of therapy should continue to reduce future health risks in testicular cancer survivors.
Figures
Similar articles
-
Italian cancer figures, report 2013: Multiple tumours.Epidemiol Prev. 2013 Jul-Oct;37(4-5 Suppl 1):1-152. Epidemiol Prev. 2013. PMID: 24259384 English, Italian.
-
Second cancers among 40,576 testicular cancer patients: focus on long-term survivors.J Natl Cancer Inst. 2005 Sep 21;97(18):1354-65. doi: 10.1093/jnci/dji278. J Natl Cancer Inst. 2005. PMID: 16174857
-
Second malignancies among survivors of germ-cell testicular cancer: a pooled analysis between 13 cancer registries.Int J Cancer. 2007 Feb 1;120(3):623-31. doi: 10.1002/ijc.22345. Int J Cancer. 2007. PMID: 17096341
-
Time trends and occupational variation in the incidence of testicular cancer in the Nordic countries.BJU Int. 2018 Sep;122(3):384-393. doi: 10.1111/bju.14148. Epub 2018 Mar 1. BJU Int. 2018. PMID: 29460991
-
Risk of second malignant neoplasms among long-term survivors of testicular cancer.J Natl Cancer Inst. 1997 Oct 1;89(19):1429-39. doi: 10.1093/jnci/89.19.1429. J Natl Cancer Inst. 1997. PMID: 9326912
Cited by
-
Second malignancies in long-term testicular cancer survivors.Int Urol Nephrol. 2014 Apr;46(4):749-56. doi: 10.1007/s11255-013-0554-4. Epub 2013 Oct 6. Int Urol Nephrol. 2014. PMID: 24096370
-
Endogenous DNA damage and testicular germ cell tumors.Int J Androl. 2009 Dec;32(6):599-606. doi: 10.1111/j.1365-2605.2008.00905.x. Epub 2008 Jul 24. Int J Androl. 2009. PMID: 18657195 Free PMC article.
-
Stage I testicular seminoma: a SEER analysis of contemporary adjuvant radiotherapy trends.J Urol. 2013 Oct;190(4):1240-4. doi: 10.1016/j.juro.2013.03.114. Epub 2013 Apr 6. J Urol. 2013. PMID: 23567749 Free PMC article.
-
Platinum exposure and cause-specific mortality among patients with testicular cancer.Cancer. 2020 Feb 1;126(3):628-639. doi: 10.1002/cncr.32538. Epub 2019 Nov 15. Cancer. 2020. PMID: 31730712 Free PMC article.
-
Comparison of non-parametric methods for ungrouping coarsely aggregated data.BMC Med Res Methodol. 2016 May 23;16:59. doi: 10.1186/s12874-016-0157-8. BMC Med Res Methodol. 2016. PMID: 27216531 Free PMC article.
References
-
- Coleman MP, Babb P, Mayer D, Quinn MJ, Sloggett A (1999) Cancer survival trends in England and Wales, 1971–1995: deprivation and NHS Region (CDROM). London: Office for National Statistics
-
- Coleman MP, Gatta G, Verdecchia A, Estève J, Sant M, Storm H, Allemani C, Ciccolallo L, Santaquilani M, Berrino F (2003) EUROCARE-3 summary: cancer survival in Europe at the end of the 20th century. Ann Oncol 14(Suppl 5): v128–v149 - PubMed
-
- Dieckmann KP, Besserer A, Loy V (1993) Low-dose radiation therapy for testicular intraepithelial neoplasia. J Cancer Res Clin Oncol 119: 355–359 - PubMed
-
- Einhorn LH, Donohue JP (1977) Chemotherapy for disseminated testicular cancer. Urol Clin North Am 4: 407–426 - PubMed
-
- Estève J, Benhamou E, Croasdale M, Raymond L (1990) Relative survival and the estimation of net survival: elements for further discussion. Stat Med 9: 529–538 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
