

Transcutaneous beta-amyloid immunization reduces cerebral beta-amyloid deposits without T cell infiltration and microhemorrhage
- PMID: 17264212
- PMCID: PMC1892920
- DOI: 10.1073/pnas.0609377104
Transcutaneous beta-amyloid immunization reduces cerebral beta-amyloid deposits without T cell infiltration and microhemorrhage
Abstract
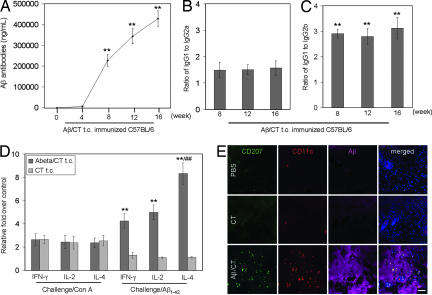
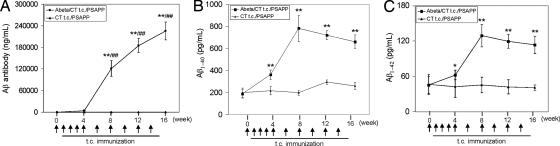
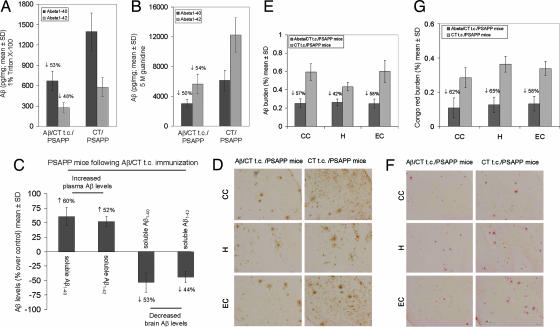
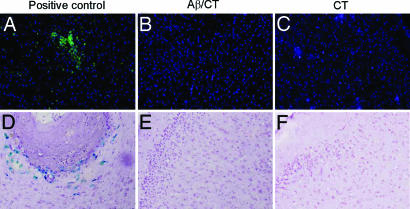
Alzheimer's disease (AD) immunotherapy accomplished by vaccination with beta-amyloid (Abeta) peptide has proved efficacious in AD mouse models. However, "active" Abeta vaccination strategies for the treatment of cerebral amyloidosis without concurrent induction of detrimental side effects are lacking. We have developed a transcutaneous (t.c.) Abeta vaccination approach and evaluated efficacy and monitored for deleterious side effects, including meningoencephalitis and microhemorrhage, in WT mice and a transgenic mouse model of AD. We demonstrate that t.c. immunization of WT mice with aggregated Abeta(1-42) plus the adjuvant cholera toxin (CT) results in high-titer Abeta antibodies (mainly of the Ig G1 class) and Abeta(1-42)-specific splenocyte immune responses. Confocal microscopy of the t.c. immunization site revealed Langerhans cells in areas of the skin containing the Abeta(1-42) immunogen, suggesting that these unique innate immune cells participate in Abeta(1-42) antigen processing. To evaluate the efficacy of t.c. immunization in reducing cerebral amyloidosis, transgenic PSAPP (APPsw, PSEN1dE9) mice were immunized with aggregated Abeta(1-42) peptide plus CT. Similar to WT mice, PSAPP mice showed high Abeta antibody titers. Most importantly, t.c. immunization with Abeta(1-42) plus CT resulted in significant decreases in cerebral Abeta(1-40,42) levels coincident with increased circulating levels of Abeta(1-40,42), suggesting brain-to-blood efflux of Abeta. Reduction in cerebral amyloidosis was not associated with deleterious side effects, including brain T cell infiltration or cerebral microhemorrhage. Together, these data suggest that t.c. immunization constitutes an effective and potentially safe treatment strategy for AD.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Vaccination of Alzheimer's model mice with Abeta derivative in alum adjuvant reduces Abeta burden without microhemorrhages.Eur J Neurosci. 2006 Nov;24(9):2530-42. doi: 10.1111/j.1460-9568.2006.05149.x. Eur J Neurosci. 2006. PMID: 17100841 Free PMC article.
-
CD40L disruption enhances Abeta vaccine-mediated reduction of cerebral amyloidosis while minimizing cerebral amyloid angiopathy and inflammation.Neurobiol Dis. 2008 Feb;29(2):336-53. doi: 10.1016/j.nbd.2007.09.009. Epub 2007 Oct 16. Neurobiol Dis. 2008. PMID: 18055209 Free PMC article.
-
Gene vaccination to bias the immune response to amyloid-beta peptide as therapy for Alzheimer disease.Arch Neurol. 2004 Dec;61(12):1859-64. doi: 10.1001/archneur.61.12.1859. Arch Neurol. 2004. PMID: 15596606 Free PMC article.
-
Amyloid-beta immunotherapy for the prevention and treatment of Alzheimer disease: lessons from mice, monkeys, and humans.Rejuvenation Res. 2006 Spring;9(1):77-84. doi: 10.1089/rej.2006.9.77. Rejuvenation Res. 2006. PMID: 16608400 Review.
-
Novel Abeta immunogens: is shorter better?Curr Alzheimer Res. 2007 Sep;4(4):427-36. doi: 10.2174/156720507781788800. Curr Alzheimer Res. 2007. PMID: 17908047 Review.
Cited by
-
The "brain-skin connection" in protein misfolding and amyloid deposits: embryological, pathophysiological, and therapeutic common grounds?Front Neurol. 2012 Apr 23;3:56. doi: 10.3389/fneur.2012.00056. eCollection 2012. Front Neurol. 2012. PMID: 22536194 Free PMC article. No abstract available.
-
Langerhans cells as targets for immunotherapy against skin cancer.Immunol Cell Biol. 2010 May-Jun;88(4):431-7. doi: 10.1038/icb.2010.31. Epub 2010 Mar 30. Immunol Cell Biol. 2010. PMID: 20351746 Free PMC article. Review.
-
Innate immunity in Alzheimer's disease: a complex affair.CNS Neurol Disord Drug Targets. 2013 Aug;12(5):593-607. doi: 10.2174/1871527311312050008. CNS Neurol Disord Drug Targets. 2013. PMID: 23574177 Free PMC article. Review.
-
Targeting S100B in Cerebral Ischemia and in Alzheimer's Disease.Cardiovasc Psychiatry Neurol. 2010;2010:687067. doi: 10.1155/2010/687067. Epub 2010 Sep 2. Cardiovasc Psychiatry Neurol. 2010. PMID: 20862385 Free PMC article.
-
Inflammaging as a prodrome to Alzheimer's disease.J Neuroinflammation. 2008 Nov 11;5:51. doi: 10.1186/1742-2094-5-51. J Neuroinflammation. 2008. PMID: 19014446 Free PMC article. Review.
References
-
- Selkoe DJ. Physiol Rev. 2001;81:741–766. - PubMed
-
- Schenk D, Barbour R, Dunn W, Gordon G, Grajeda H, Guido T, Hu K, Huang J, Johnson-Wood K, Khan K, et al. Nature. 1999;400:173–177. - PubMed
-
- Bayer AJ, Bullock R, Jones RW, Wilkinson D, Paterson KR, Jenkins L, Millais SB, Donoghue S. Neurology. 2005;64:94–101. - PubMed
-
- Hock C, Konietzko U, Streffer JR, Tracy J, Signorell A, Muller-Tillmanns B, Lemke U, Henke K, Moritz E, Garcia E, et al. Neuron. 2003;38:547–554. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
