

Acute deep hand burns covered by a pocket flap-graft: long-term outcome based on nine cases
- PMID: 17268577
- PMCID: PMC1781957
Acute deep hand burns covered by a pocket flap-graft: long-term outcome based on nine cases
Abstract
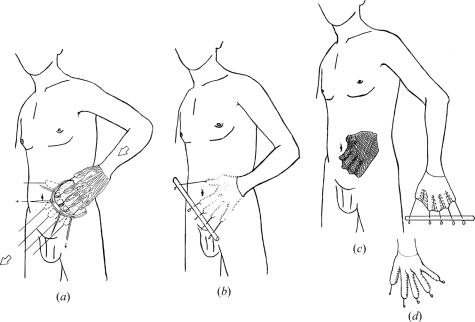
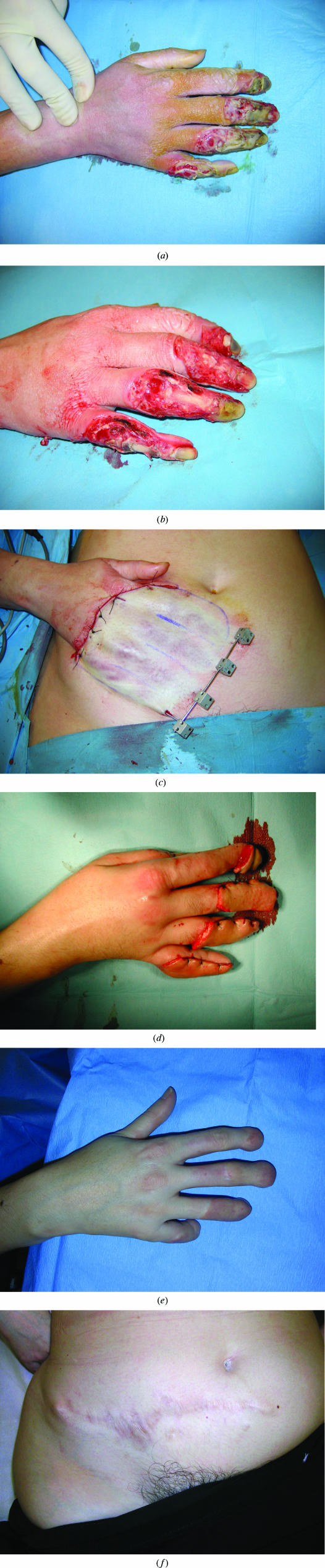
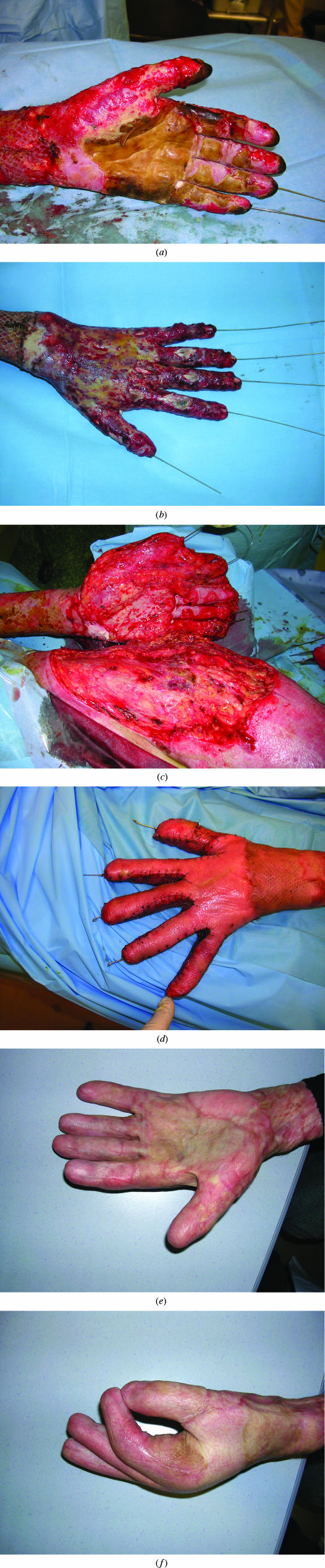
Objective: We evaluated the long-term outcome of the "pocket flap-graft" technique, used to cover acute deep burns of the dorsum of the hand, and analyzed surgical alternatives.
Methods: This was a 6-year, retrospective study of 8 patients with extensive burns and 1 patient with a single burn (11 hands in all) treated by defatted abdominal wall pockets. We studied the medical records of the patients, and conducted a follow-up examination.
Results: All hands had fourth-degree thermal burns caused by flames, with exposure of tendons, bones, and joints, and poor functional prognosis. One third of patients had multiple injuries. Burns affected an average of 36% of the hand surface, and mean coverage was 92.8 cm(2). One patient died. The 8 others were seen at 30-month follow-up: the skin quality of the flap was found to be good in 55% of the cases, the score on the Vancouver Scar Scale was 2.4, the Kapandji score was 4.5, and total active motion was 37% of that of a normal hand. Hand function was limited in only 2 cases, 8 patients were able to drive, and 3 patients had gone back to work.
Conclusion: The pocket flap-graft allows preservation of hand function following severe burns, when local or free flaps are impossible to perform. Debulking of the flap at the time of elevation limits the need for secondary procedures.
Figures


References
-
- Sheridan RL, Hurley J, Smith MA, et al. The acutely burned hand: management and outcome based on a ten-year experience with 1047 acute hand burns. J Trauma. 1995;38(3):406–411. - PubMed
-
- Baux S. Les brûlures. In: Tubiana R, editor. Traité de chirurgie de la main Tome 3. Paris: Masson; 1986. pp. 648–672.
-
- Heifland A, Piatkowski A, Noah EM, Pallua N. Update on the use of collagen/glycosaminoglycate skin substitute---six years of experiences with artificial skin in 15 German burn centers. Burns. 2004;30(5):471–475. - PubMed
-
- Nuchtern JG, Engrav LH, Nakamura DY, Dutcher KA, Heimbach DM, Vedder NB. Treatment of fourth-degree hand burns. J Burn Care Rehabil. 1995;16(1):36–42. - PubMed
-
- Voulliaume D, Mojallal A, Comparin JP, Foyatier JL. Severe hand burns and flaps: indications. Ann Chir Plast Esthet. 2005;50(4):314–319. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources