

Factors associated with treatment for hypotension in extremely low gestational age newborns during the first postnatal week
- PMID: 17272616
- PMCID: PMC2803046
- DOI: 10.1542/peds.2006-1138
Factors associated with treatment for hypotension in extremely low gestational age newborns during the first postnatal week
Abstract
Objective: The goals were to identify the blood pressures of extremely low gestational age newborns that prompt intervention, to identify other infant characteristics associated with receipt of therapies intended to increase blood pressure, and to assess the interinstitutional variability in the use of these therapies.
Methods: The cohort included 1507 extremely low gestational age newborns born at 23 weeks to 27 weeks of gestation, at 14 institutions, between March 2002 and August 2004; 1387 survived the first postnatal week. Blood pressures were measured as clinically indicated. Interventions were grouped as any treatment (ie, vasopressor and/or fluid boluses of >10 mL/kg) and vasopressor treatment, and logistic regression analyses were performed.
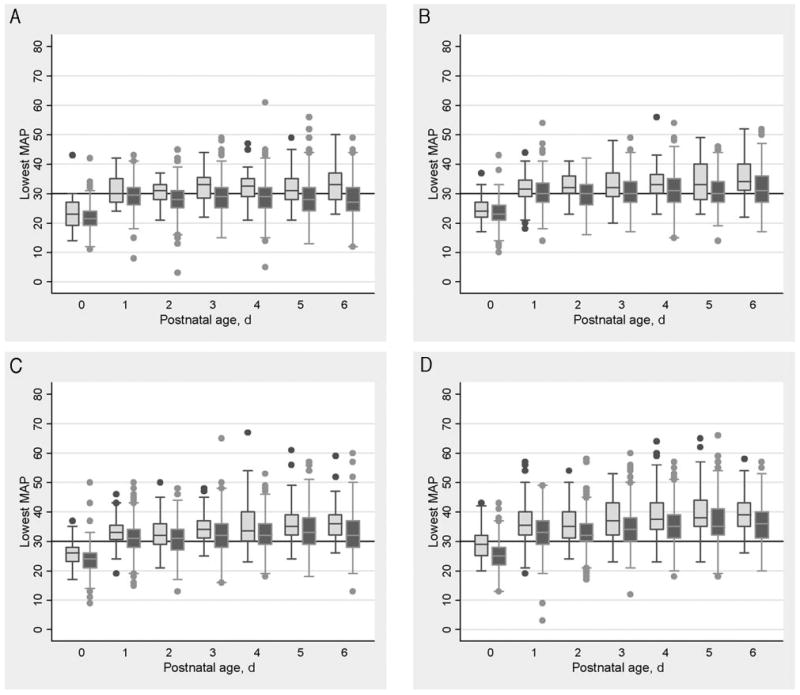
Results: At each gestational age, the lowest mean arterial pressures in treated and untreated infants tended to increase with advancing postnatal age. Infants who received any therapy tended to have lower mean arterial pressures than infants who did not, but uniform thresholds for treatment were not apparent. The proportion of infants receiving any treatment decreased with increasing gestational age from 93% at 23 weeks to 73% at 27 weeks. Treatment nearly always began during the first 24 hours of life. Lower gestational age, lower birth weight, male gender, and higher Score for Neonatal Acute Physiology-II values were associated with any treatment and vasopressor treatment. Institutions varied greatly in their tendency to offer any treatment and vasopressor treatment. Neither the lowest mean arterial pressure on the day of treatment nor other characteristics of the infants accounted for center differences in treatment.
Conclusions: Blood pressure in extremely premature infants not treated for hypotension increased directly with both increasing gestational age and postnatal age. The decision to provide treatment was associated more strongly with the center where care was provided than with infant attributes.
Figures
Comment in
-
Time for pressure tactics.Pediatrics. 2007 Feb;119(2):396-7. doi: 10.1542/peds.2006-3456. Pediatrics. 2007. PMID: 17272628 No abstract available.
References
-
- Osborn DA. Diagnosis and treatment of preterm transitional circulatory compromise. Early Hum Dev. 2005;81:413–422. - PubMed
-
- Martens SE, Rijken M, Stoelhorst GM, et al. Is hypotension a major risk factor for neurological morbidity at term age in very preterm infants? Early Hum Dev. 2003;75:79–89. - PubMed
-
- Kluckow M, Evans N. Low systemic blood flow in the preterm infant. Semin Neonatol. 2001;6:75–84. - PubMed
-
- Pladys P, Wodey E, Beuchee A, Branger B, Betremieux P. Left ventricle output and mean arterial blood pressure in preterm infants during the 1st day of life. Eur J Pediatr. 1999;158:817–824. - PubMed
-
- Lopez SL, Leighton JO, Walther FJ. Supranormal cardiac output in the dopamine- and dobutamine-dependent preterm infant. Pediatr Cardiol. 1997;18:292–296. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
