

Calcification of human articular knee cartilage is primarily an effect of aging rather than osteoarthritis
- PMID: 17276093
- PMCID: PMC2707182
- DOI: 10.1016/j.joca.2006.10.017
Calcification of human articular knee cartilage is primarily an effect of aging rather than osteoarthritis
Erratum in
- Osteoarthritis Cartilage. 2009 Apr;17(4):556
Abstract
Objective: Pathologic calcification of articular cartilage in human knees is often associated with advanced age and conditions of osteoarthritis (OA). Coincidently, most studies that have characterized calcification in joint cartilage have examined populations that are aged and presenting with clinical symptoms. Generally, these studies rely upon relatively insensitive plain radiographs or synovial fluid crystal analyses to quantify calcium levels. The purpose of this study was to examine the relationship between cartilage calcification and aging in an unselected donor population of diverse age using highly sensitive calcification imaging.
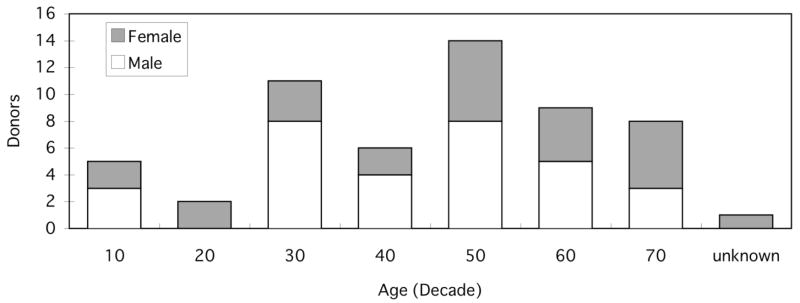
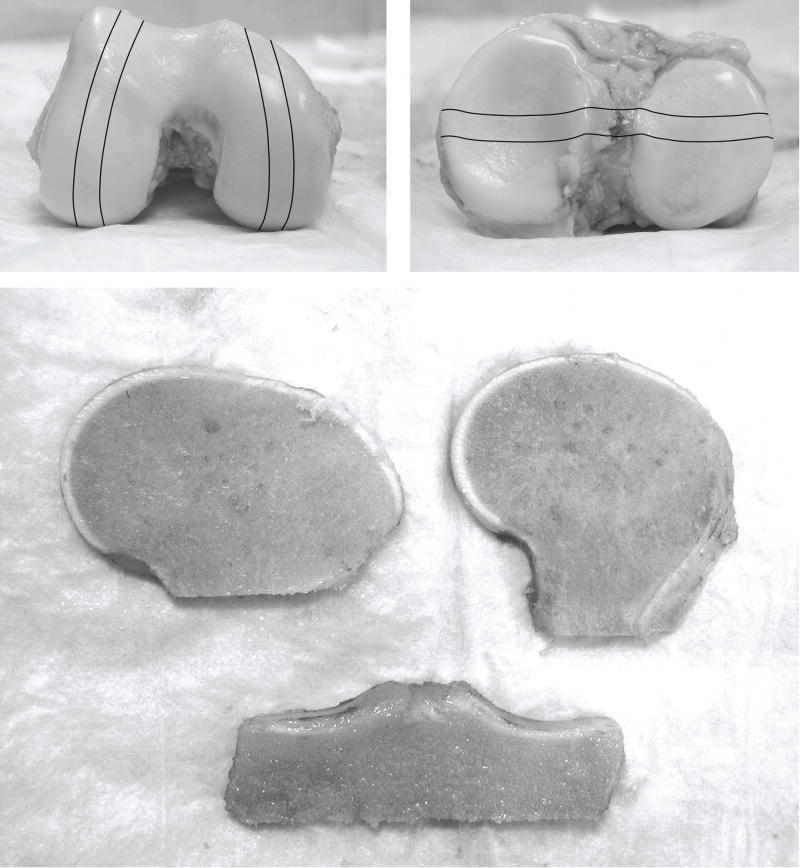
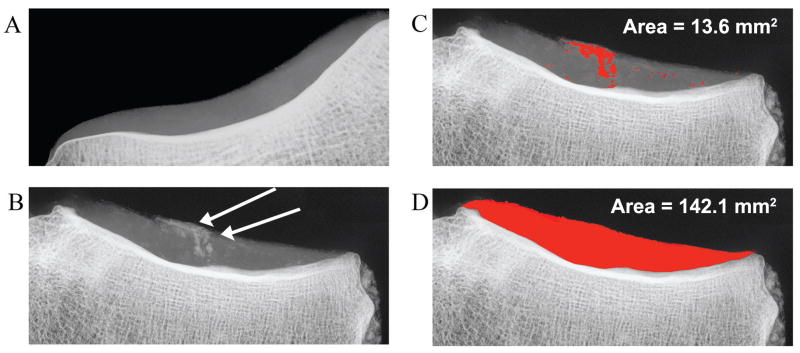
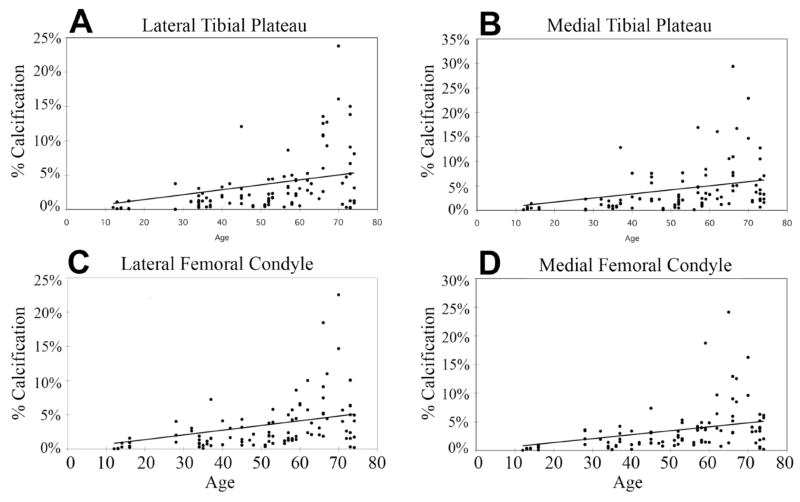
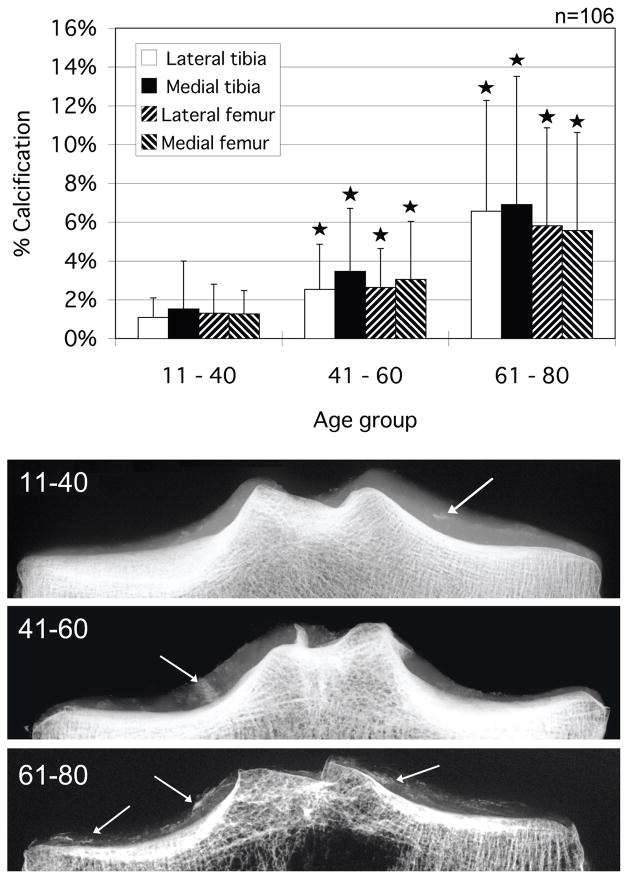
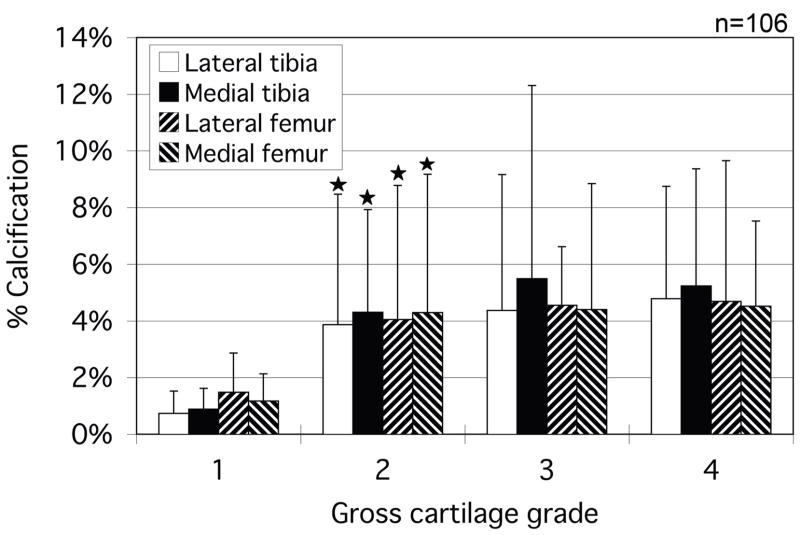
Methods: A group of 106 knee blocks were obtained from 56 individual donors (25 females and 31 males, aged 12-74, avg. 50.3 years). Condylar surfaces were graded on a 4-point OA grading scale for cartilage degeneration. The condyles were cut into approximately 7-10mm thick slabs. Using a Faxitron radiography system, high-resolution images were taken of the slabs to specifically image calcification in cartilage. The quantified calcification areas were then analyzed and correlations with both OA grade and age were assessed.
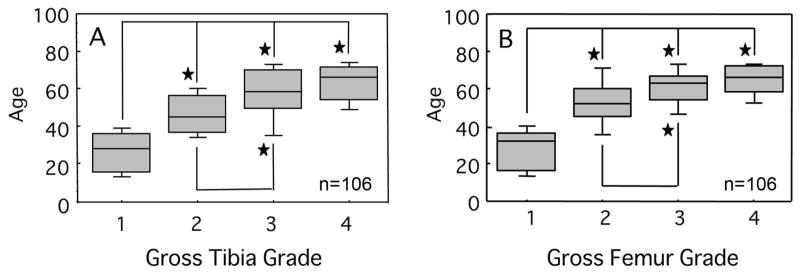
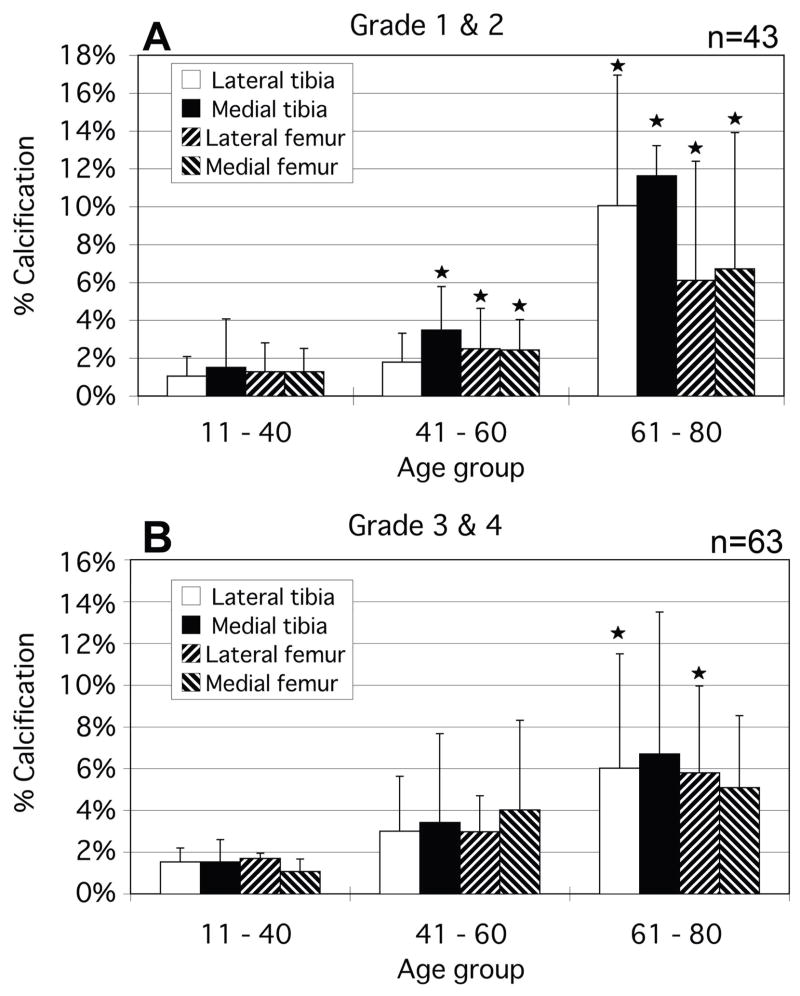
Results: Every knee presented some measurable calcification. The relative calcium deposition had a significant positive correlation with age. This same positive correlation was seen between condyles showing grade 1 and 2 changes. OA grades higher than 2 did not present any further significant increase in calcium levels.
Conclusion: These observations indicate that age rather than OA is the predominant factor driving progressive pathologic calcification in articular cartilage.
Figures
References
-
- Abyad A, Boyer JT. Arthritis and aging. Curr Opin Rheumatol. 1992;4(2):153–9. - PubMed
-
- Derfus BA, Kurian JB, Butler JJ, Daft LJ, Carrera GF, Ryan LM, et al. The high prevalence of pathologic calcium crystals in pre-operative knees. J Rheumatol. 2002;29(3):570–4. - PubMed
-
- Yang BY, Sartoris DJ, Resnick D, Clopton P. Calcium pyrophosphate dihydrate crystal deposition disease: frequency of tendon calcification about the knee. J Rheumatol. 1996;23(5):883–8. - PubMed
-
- Canhao H, Fonseca JE, Leandro MJ, Romeu JC, Pimentao JB, Costa JT, Queiroz MV. Cross-sectional study of 50 patients with calcium pyrophosphate dihydrate crystal arthropathy. Clin Rheumatol. 2001;20(2):119–22. - PubMed
-
- Abreu M, Johnson K, Chung CB, De Lima JE, Jr, Trudell D, Terkeltaub R, et al. Calcification in calcium pyrophosphate dihydrate (CPPD) crystalline deposits in the knee: anatomic, radiographic, MR imaging, and histologic study in cadavers. Skeletal Radiol. 2004;33(7):392–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
