

MRI of the breast for the detection and assessment of the size of ductal carcinoma in situ
- PMID: 17277561
- PMCID: PMC2626696
- DOI: 10.3348/kjr.2007.8.1.32
MRI of the breast for the detection and assessment of the size of ductal carcinoma in situ
Abstract
Objective: The aim of the study was to compare the accuracy of magnetic resonance imaging (MRI) and mammography for the detection and assessment of the size of ductal carcinoma in situ (DCIS).
Materials and methods: The preoperative contrast-enhanced MRI and mammography were analyzed in respect of the detection and assessment of the size of DCIS in 72 patients (age range: 30-67 years, mean age: 47 years). The MRI and mammographic measurements were compared with the histopathologic size with using the Pearson's correlation coefficients and the Mann-Whitney u test. We evaluated whether the breast density, the tumor nuclear grade, the presence of comedo necrosis and microinvasion influenced the MRI and mammographic size estimates by using the chi-square test.
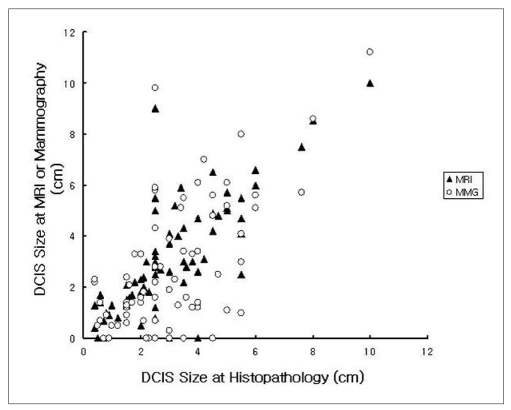
Results: Of the 72 DCIS lesions, 68 (94%) were detected by MRI and 62 (86%) were detected by mammography. Overall, the Pearson's correlation of the size between MRI and histopathology was 0.786 versus 0.633 between mammography and histopathology (p < 0.001). MRI underestimated the size by more than 1 cm (including false negative examination) in 12 patients (17%), was accurate in 52 patients (72%) and overestimated the size by more than 1 cm in eight patients (11%) whereas mammography underestimated the size in 25 patients (35%), was accurate in 31 patients (43%) and overestimated the size in 16 patients (22%). The MRI, but not the mammography, showed significant correlation for the assessment of the size of tumor in noncomedo DCIS (p < 0.001 vs p = 0.060). The assessment of tumor size by MRI was affected by the nuclear grade (p = 0.008) and the presence of comedo necrosis (p = 0.029), but not by the breast density (p = 0.747) or microinvasion (p = 0.093).
Conclusion: MRI was more accurate for the detection and assessment of the size of DCIS than mammography.
Figures
Similar articles
-
The value of magnetic resonance imaging in diagnosis and size assessment of in situ and small invasive breast carcinoma.Am J Surg. 2006 Aug;192(2):172-8. doi: 10.1016/j.amjsurg.2006.02.026. Am J Surg. 2006. PMID: 16860625
-
MR features to suggest microinvasive ductal carcinoma of the breast: can it be differentiated from pure DCIS?Acta Radiol. 2013 Sep;54(7):742-8. doi: 10.1177/0284185113484640. Epub 2013 Apr 30. Acta Radiol. 2013. PMID: 23588154
-
Diagnostic accuracy of mammography, clinical examination, US, and MR imaging in preoperative assessment of breast cancer.Radiology. 2004 Dec;233(3):830-49. doi: 10.1148/radiol.2333031484. Epub 2004 Oct 14. Radiology. 2004. PMID: 15486214
-
Ductal carcinoma in situ of the breast: MR imaging findings with histopathologic correlation.Radiographics. 2010 Oct;30(6):1673-87. doi: 10.1148/rg.306105510. Radiographics. 2010. PMID: 21071382 Review.
-
Potential role of magnetic resonance imaging and other modalities in ductal carcinoma in situ detection.Magn Reson Imaging Clin N Am. 2001 May;9(2):345-56, vii. Magn Reson Imaging Clin N Am. 2001. PMID: 11493424 Review.
Cited by
-
Identifying recurrences and metastasis after ductal carcinoma in situ (DCIS) of the breast.Histopathology. 2023 Jan;82(1):106-118. doi: 10.1111/his.14804. Histopathology. 2023. PMID: 36482277 Free PMC article. Review.
-
The adjacent vessel sign on breast MRI: new data and a subgroup analysis for 1,084 histologically verified cases.Korean J Radiol. 2010 Mar-Apr;11(2):178-86. doi: 10.3348/kjr.2010.11.2.178. Epub 2010 Feb 22. Korean J Radiol. 2010. PMID: 20191065 Free PMC article.
-
Value of pre-operative breast MRI for the size assessment of ductal carcinoma in situ.Br J Radiol. 2016;89(1058):20150543. doi: 10.1259/bjr.20150543. Epub 2015 Nov 16. Br J Radiol. 2016. PMID: 26568438 Free PMC article.
-
Radiological and pathological size estimations of pure ductal carcinoma in situ of the breast, specimen handling and the influence on the success of breast conservation surgery: a review of 2564 cases from the Sloane Project.Br J Cancer. 2010 Jan 19;102(2):285-93. doi: 10.1038/sj.bjc.6605513. Epub 2010 Jan 5. Br J Cancer. 2010. PMID: 20051953 Free PMC article.
-
Probability of malignancy for lesions detected on breast MRI: a predictive model incorporating BI-RADS imaging features and patient characteristics.Eur Radiol. 2011 Aug;21(8):1609-17. doi: 10.1007/s00330-011-2094-6. Epub 2011 Feb 27. Eur Radiol. 2011. PMID: 21359910
References
-
- Dershaw DD, Abramson A, Kinne DW. Ductal carcinoma in situ: mammographic findings and clinical implications. Radiology. 1989;170:411–415. - PubMed
-
- Stomper PC, Connolly JL, Meyer JE, Harris JR. Clinically occult ductal carcinoma in situ detected with mammography: analysis of 100 cases with radiologic-pathologic correlation. Radiology. 1989;172:235–241. - PubMed
-
- Ikeda DM, Andersson I. Ductal carcinoma in situ (DCIS): atypical mammographic appearances. Radiology. 1989;172:661–666. - PubMed
-
- Silverstein MJ. Ductal carcinoma in situ (DCIS) of the breast: diagnostic and therapeutic controversies. J Am Coll Surg. 2001;192:196–214. - PubMed
-
- Orel SG, Schnall MD, LiVolsi VA, Troupin RH. Suspicious breast lesions: MR imaging with radiologic-pathologic correlation. Radiology. 1994;190:485–493. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
