

Targeted social distancing design for pandemic influenza
- PMID: 17283616
- PMCID: PMC3372334
- DOI: 10.3201/eid1211.060255
Targeted social distancing design for pandemic influenza
Abstract
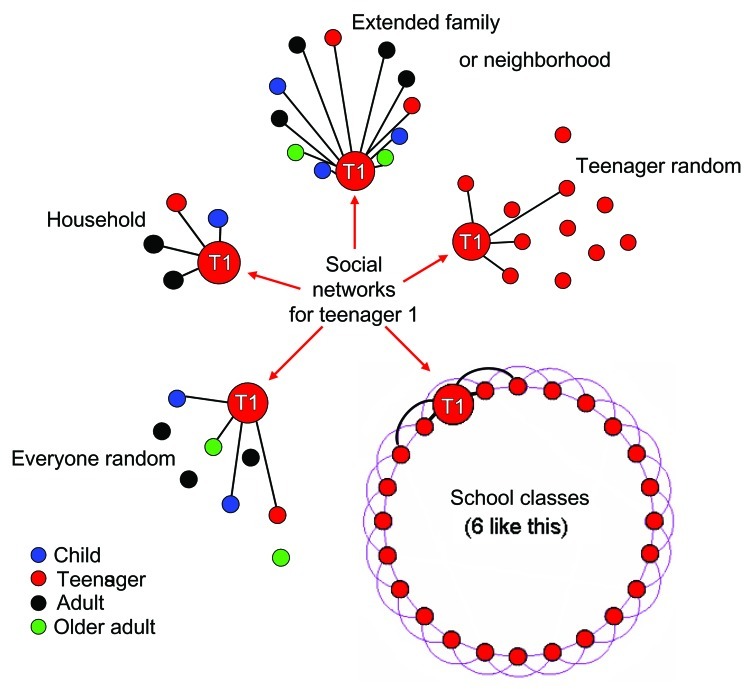
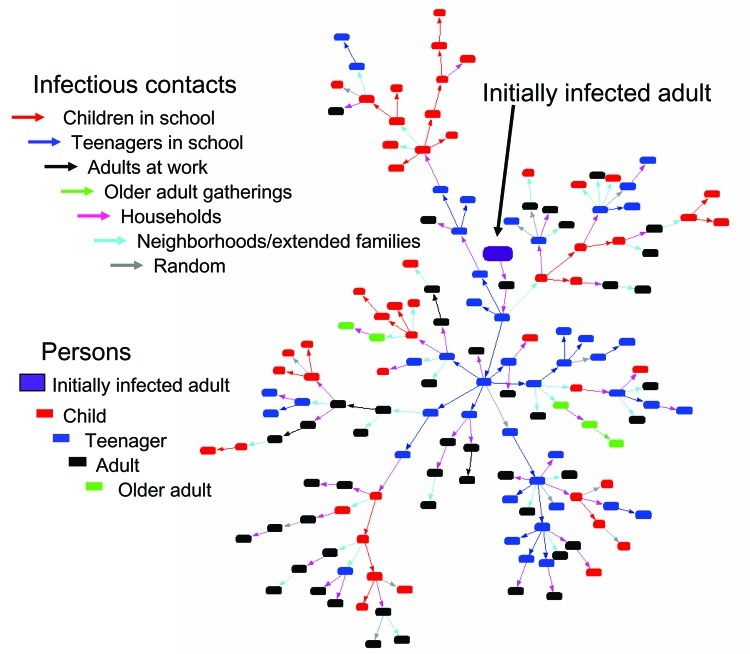
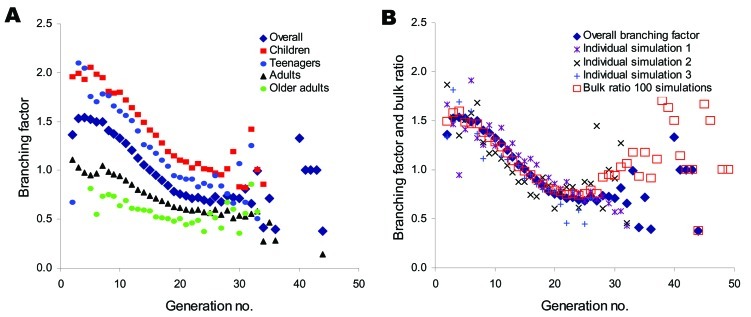
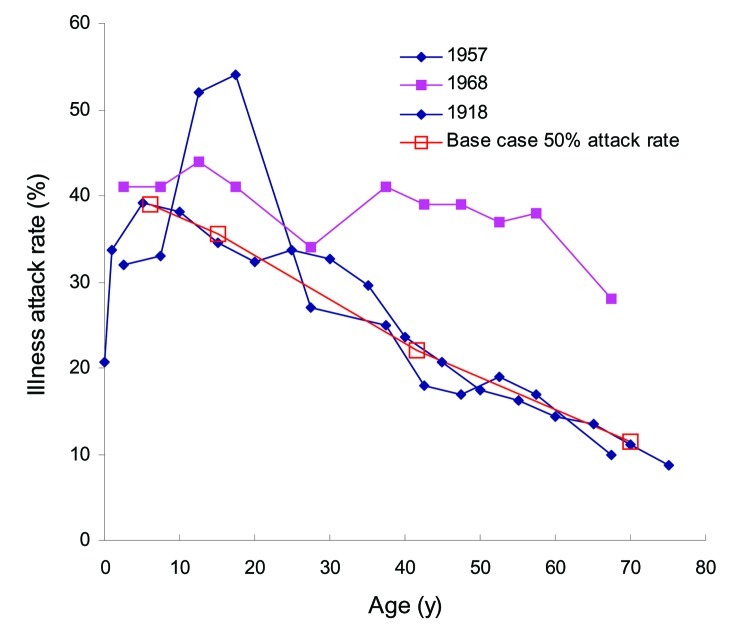
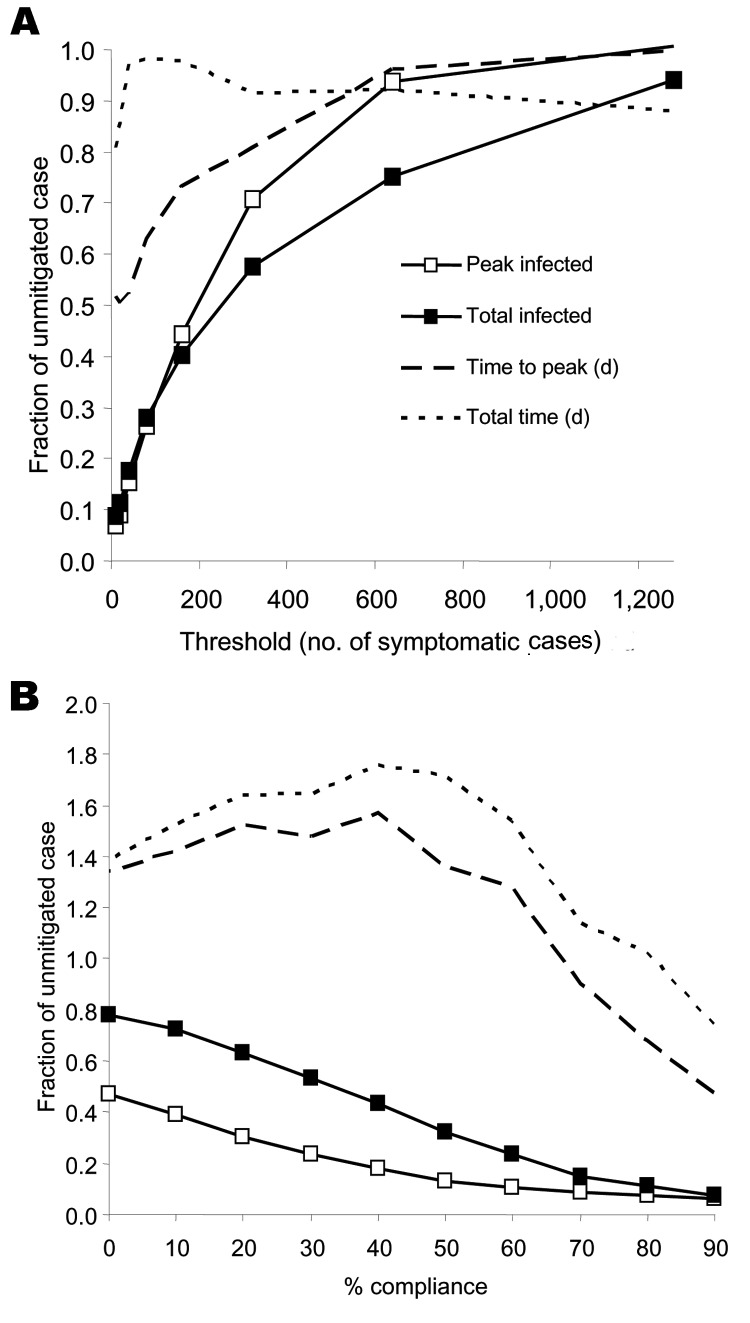
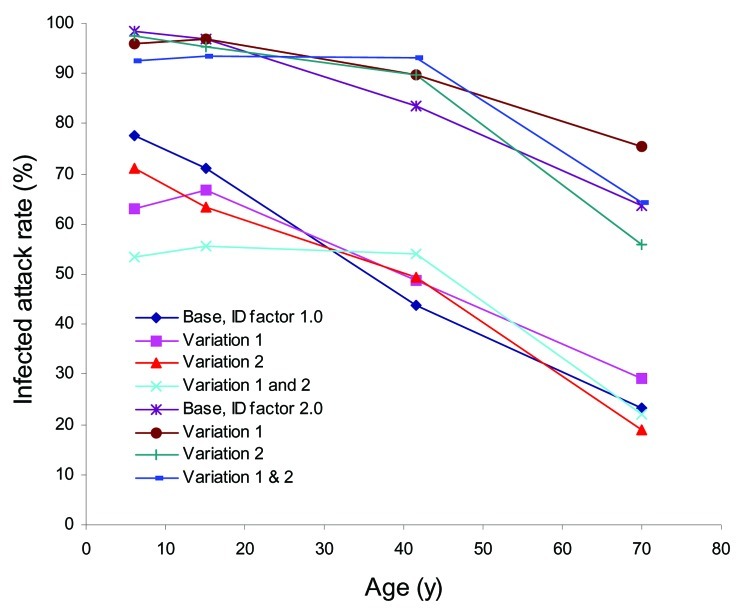
Targeted social distancing to mitigate pandemic influenza can be designed through simulation of influenza's spread within local community social contact networks. We demonstrate this design for a stylized community representative of a small town in the United States. The critical importance of children and teenagers in transmission of influenza is first identified and targeted. For influenza as infectious as 1957-58 Asian flu (=50% infected), closing schools and keeping children and teenagers at home reduced the attack rate by >90%. For more infectious strains, or transmission that is less focused on the young, adults and the work environment must also be targeted. Tailored to specific communities across the world, such design would yield local defenses against a highly virulent strain in the absence of vaccine and antiviral drugs.
Figures
References
-
- World Health Organization. Avian influenza frequently asked questions. Geneva: The Organization; 2005. - PubMed
-
- US Homeland Security Council. National strategy for pandemic influenza: implementation plan. Washington: US Department of Homeland Security; 2006.
-
- US Department of Health and Human Services. Pandemic influenza plan HHS. Washington: The Department; 2005.
-
- Glass RJ, Glass LM, Beyeler WE. Local mitigation strategies for pandemic influenza: prepared for the Department of Homeland Security under the National Infrastructure Simulation and Analysis Center. Report no. SAND2005–7955J. Washington: Department of Homeland Security; 2005.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical