

Forced mobilization accelerates pathogenesis: characterization of a preclinical surgical model of osteoarthritis
- PMID: 17284317
- PMCID: PMC1860072
- DOI: 10.1186/ar2120
Forced mobilization accelerates pathogenesis: characterization of a preclinical surgical model of osteoarthritis
Erratum in
- Arthritis Res Ther. 2008;10(5):407
Abstract
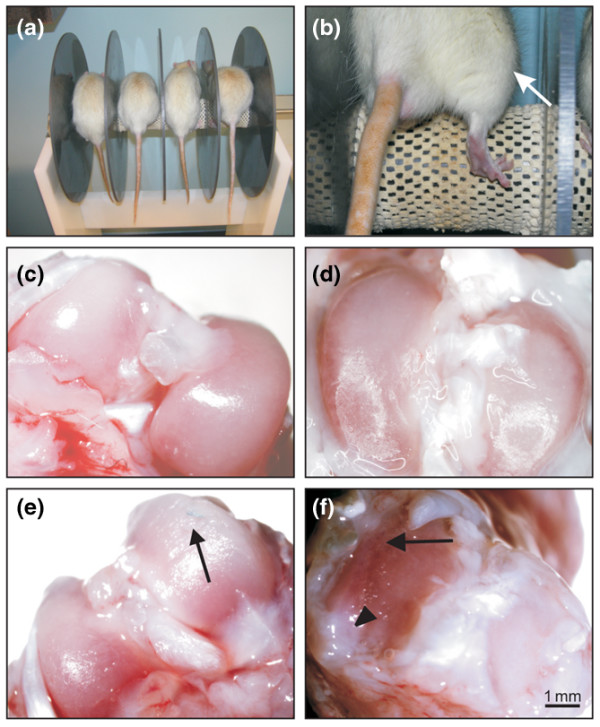
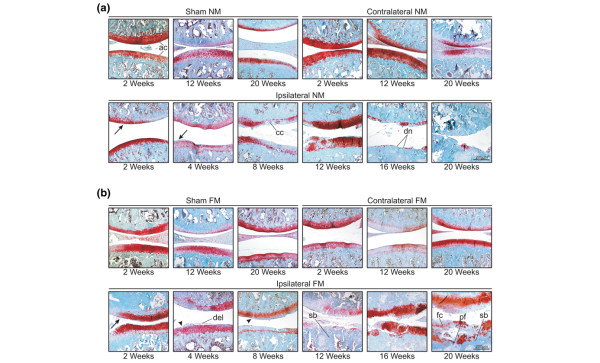
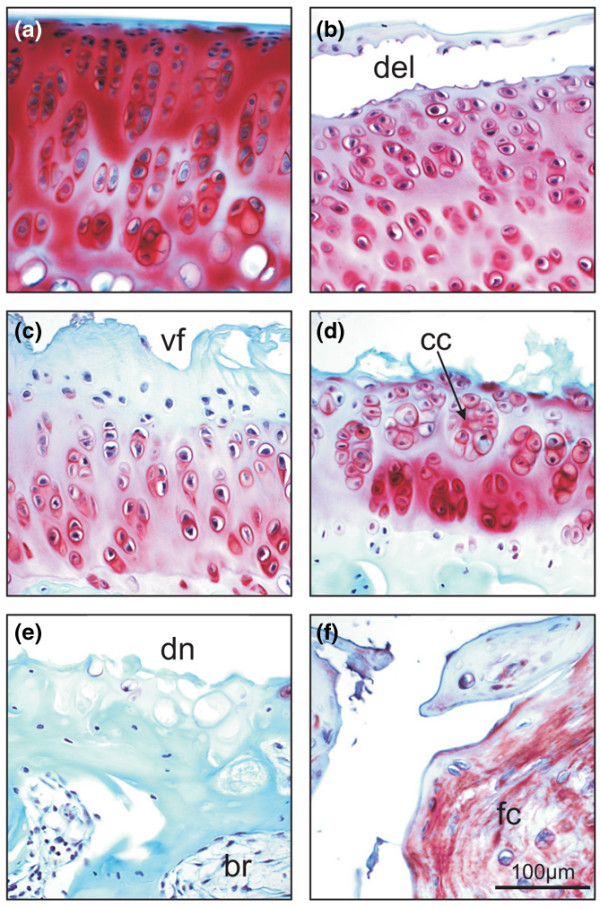
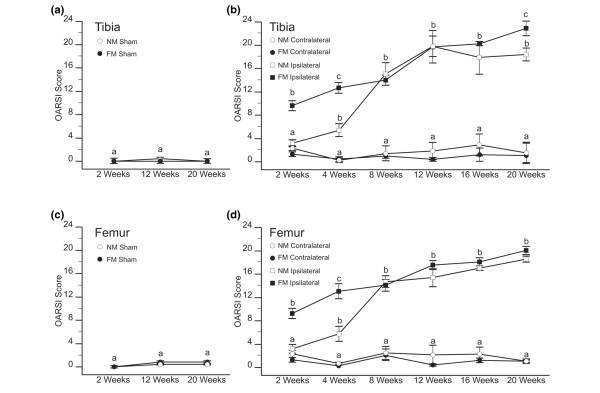
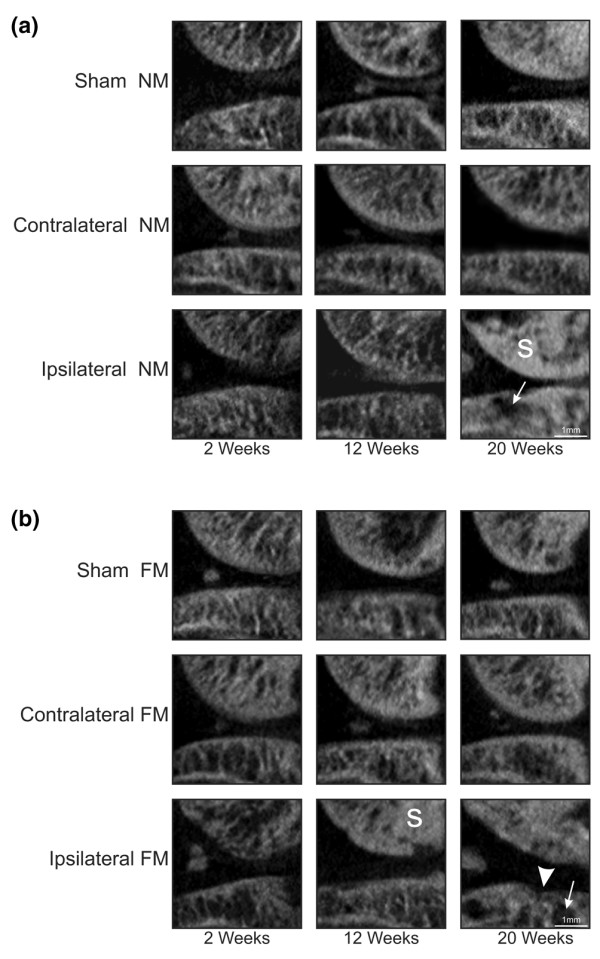
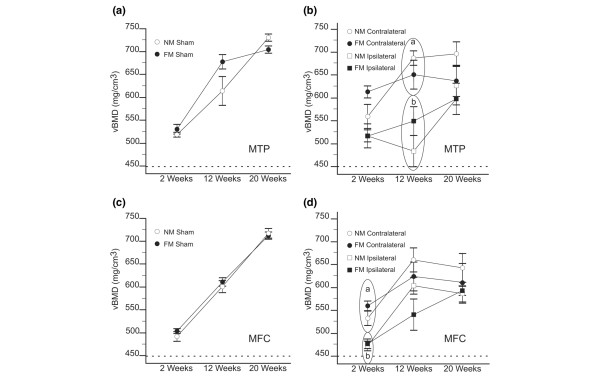
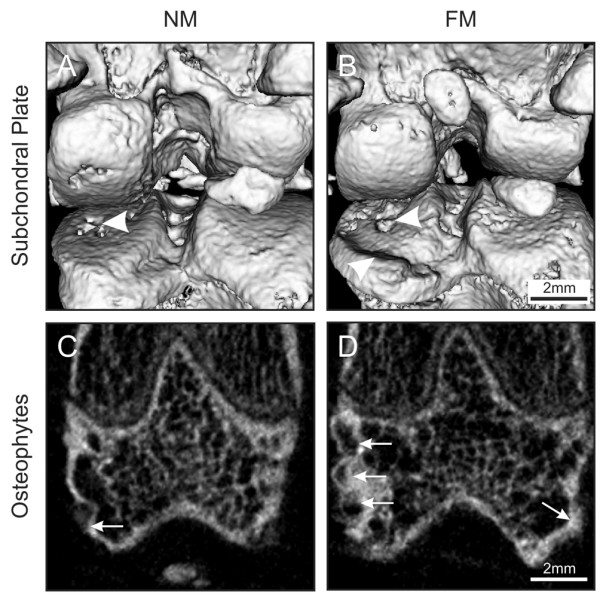
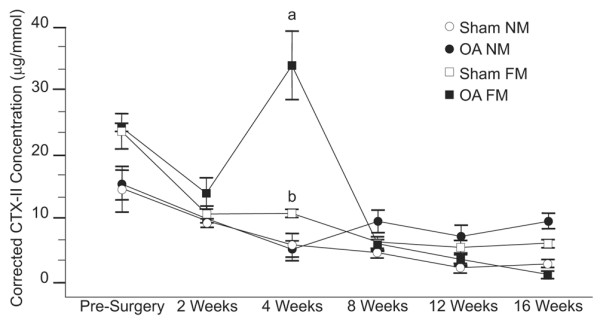
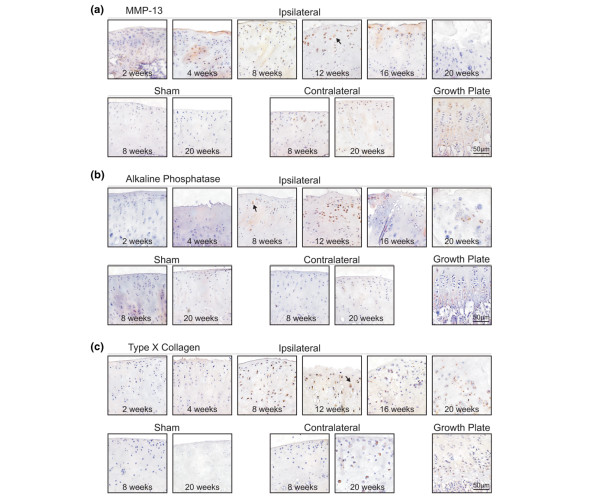
Preclinical osteoarthritis (OA) models are often employed in studies investigating disease-modifying OA drugs (DMOADs). In this study we present a comprehensive, longitudinal evaluation of OA pathogenesis in a rat model of OA, including histologic and biochemical analyses of articular cartilage degradation and assessment of subchondral bone sclerosis. Male Sprague-Dawley rats underwent joint destabilization surgery by anterior cruciate ligament transection and partial medial meniscectomy. The contralateral joint was evaluated as a secondary treatment, and sham surgery was performed in a separate group of animals (controls). Furthermore, the effects of walking on a rotating cylinder (to force mobilization of the joint) on OA pathogenesis were assessed. Destabilization-induced OA was investigated at several time points up to 20 weeks after surgery using Osteoarthritis Research Society International histopathology scores, in vivo micro-computed tomography (CT) volumetric bone mineral density analysis, and biochemical analysis of type II collagen breakdown using the CTX II biomarker. Expression of hypertrophic chondrocyte markers was also assessed in articular cartilage. Cartilage degradation, subchondral changes, and subchondral bone loss were observed as early as 2 weeks after surgery, with considerable correlation to that seen in human OA. We found excellent correlation between histologic changes and micro-CT analysis of underlying bone, which reflected properties of human OA, and identified additional molecular changes that enhance our understanding of OA pathogenesis. Interestingly, forced mobilization exercise accelerated OA progression. Minor OA activity was also observed in the contralateral joint, including proteoglycan loss. Finally, we observed increased chondrocyte hypertrophy during pathogenesis. We conclude that forced mobilization accelerates OA damage in the destabilized joint. This surgical model of OA with forced mobilization is suitable for longitudinal preclinical studies, and it is well adapted for investigation of both early and late stages of OA. The time course of OA progression can be modulated through the use of forced mobilization.
Figures
References
-
- Altman R, Asch E, Bloch D, Bole G, Borenstein D, Brandt K, Christy W, Cooke TD, Greenwald R, Hochberg M, et al. Development of criteria for the classification and reporting of osteoarthritis. Classification of osteoarthritis of the knee. Diagnostic and Therapeutic Criteria Committee of the American Rheumatism Association. Arthritis Rheum. 1986;29:1039–1049. doi: 10.1002/art.1780290816. - DOI - PubMed
-
- Mandelbaum B, Waddell D. Etiology and pathophysiology of osteoarthritis. Orthopedics. 2005;28:s207–s214. - PubMed
-
- Blumenkrantz G, Lindsey CT, Dunn TC, Jin H, Ries MD, Link TM, Steinbach LS, Majumdar S. A pilot, two-year longitudinal study of the interrelationship between trabecular bone and articular cartilage in the osteoarthritic knee. Osteoarthritis Cartilage. 2004;12:997–1005. doi: 10.1016/j.joca.2004.09.001. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
