

Non-rigid alignment of pre-operative MRI, fMRI, and DT-MRI with intra-operative MRI for enhanced visualization and navigation in image-guided neurosurgery
- PMID: 17289403
- PMCID: PMC3358788
- DOI: 10.1016/j.neuroimage.2006.11.060
Non-rigid alignment of pre-operative MRI, fMRI, and DT-MRI with intra-operative MRI for enhanced visualization and navigation in image-guided neurosurgery
Abstract
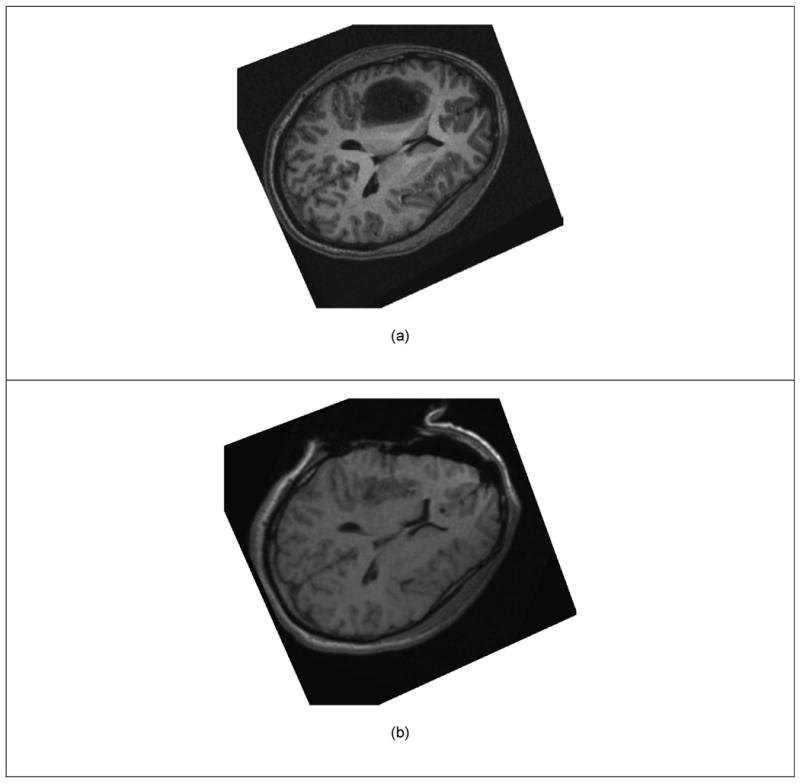
Objective: The usefulness of neurosurgical navigation with current visualizations is seriously compromised by brain shift, which inevitably occurs during the course of the operation, significantly degrading the precise alignment between the pre-operative MR data and the intra-operative shape of the brain. Our objectives were (i) to evaluate the feasibility of non-rigid registration that compensates for the brain deformations within the time constraints imposed by neurosurgery, and (ii) to create augmented reality visualizations of critical structural and functional brain regions during neurosurgery using pre-operatively acquired fMRI and DT-MRI.
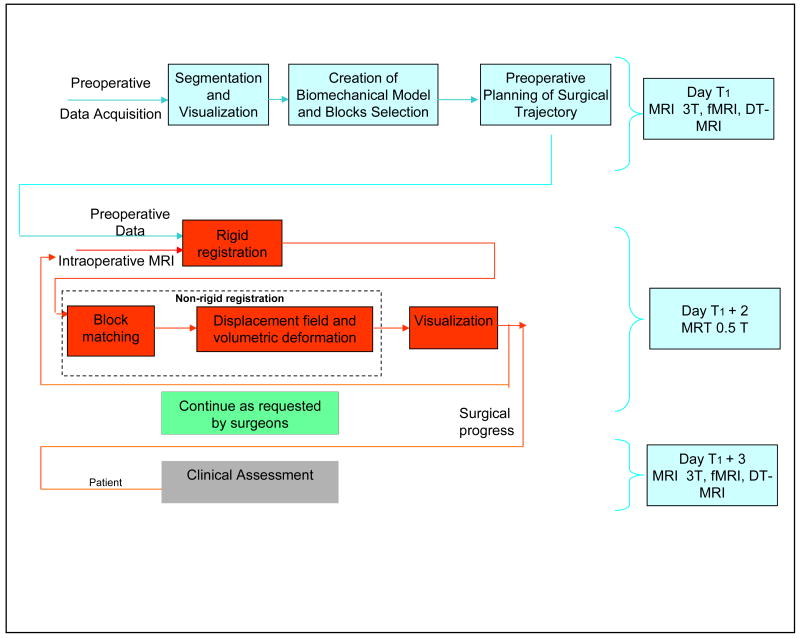
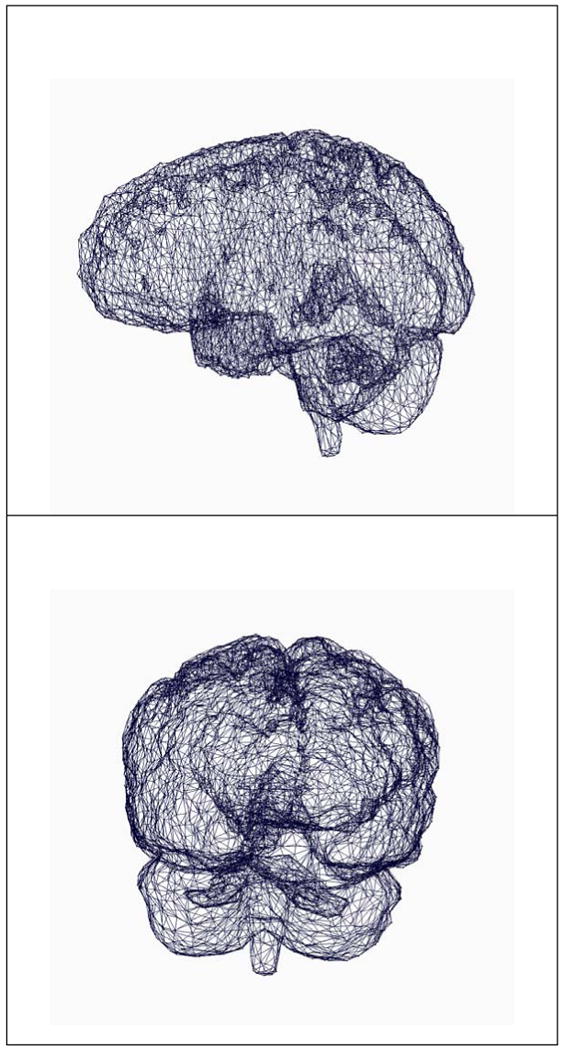
Materials and methods: Eleven consecutive patients with supratentorial gliomas were included in our study. All underwent surgery at our intra-operative MR imaging-guided therapy facility and have tumors in eloquent brain areas (e.g. precentral gyrus and cortico-spinal tract). Functional MRI and DT-MRI, together with MPRAGE and T2w structural MRI were acquired at 3 T prior to surgery. SPGR and T2w images were acquired with a 0.5 T magnet during each procedure. Quantitative assessment of the alignment accuracy was carried out and compared with current state-of-the-art systems based only on rigid registration.
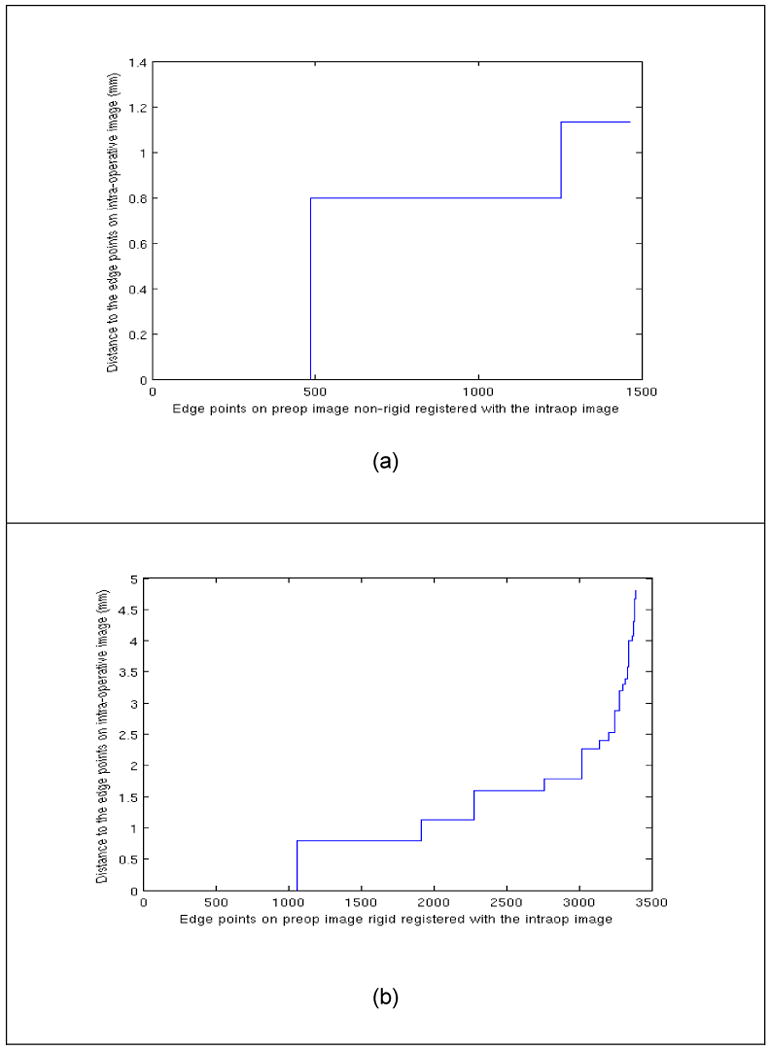
Results: Alignment between pre-operative and intra-operative datasets was successfully carried out during surgery for all patients. Overall, the mean residual displacement remaining after non-rigid registration was 1.82 mm. There is a statistically significant improvement in alignment accuracy utilizing our non-rigid registration in comparison to the currently used technology (p<0.001).
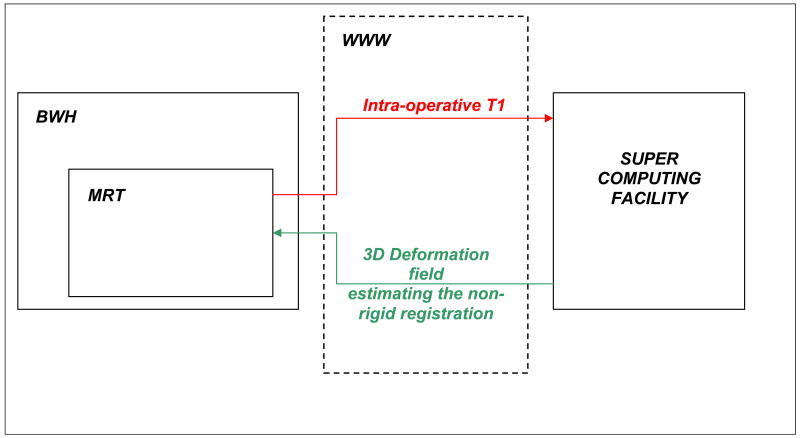
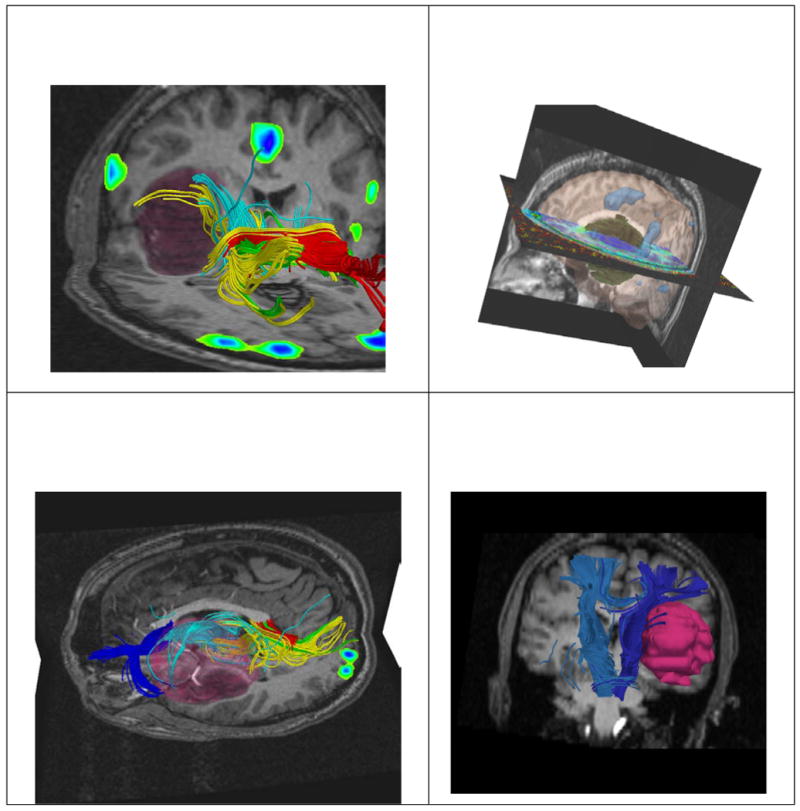
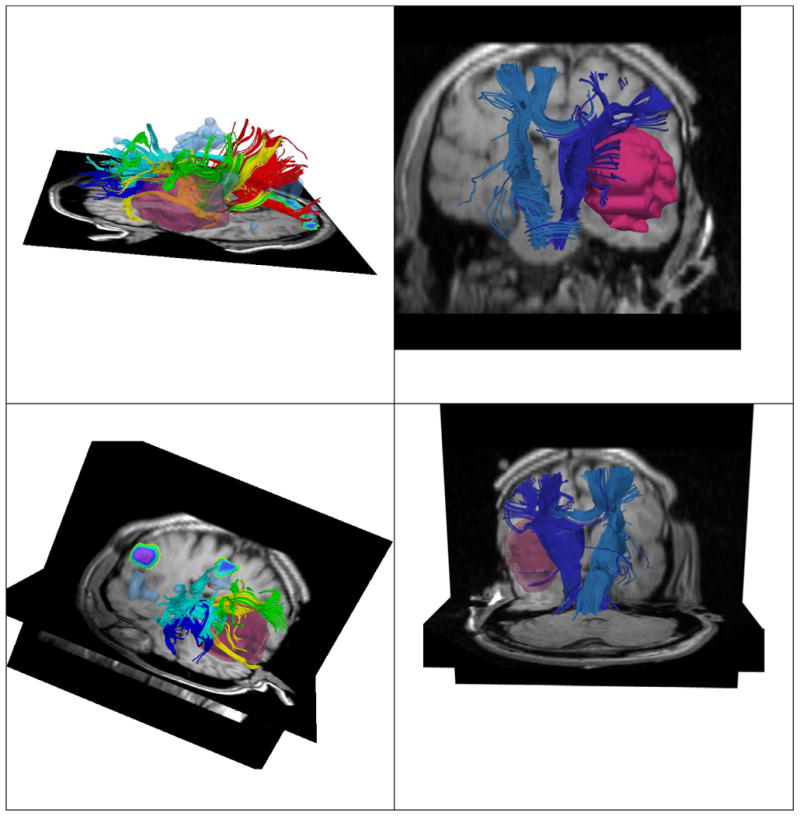
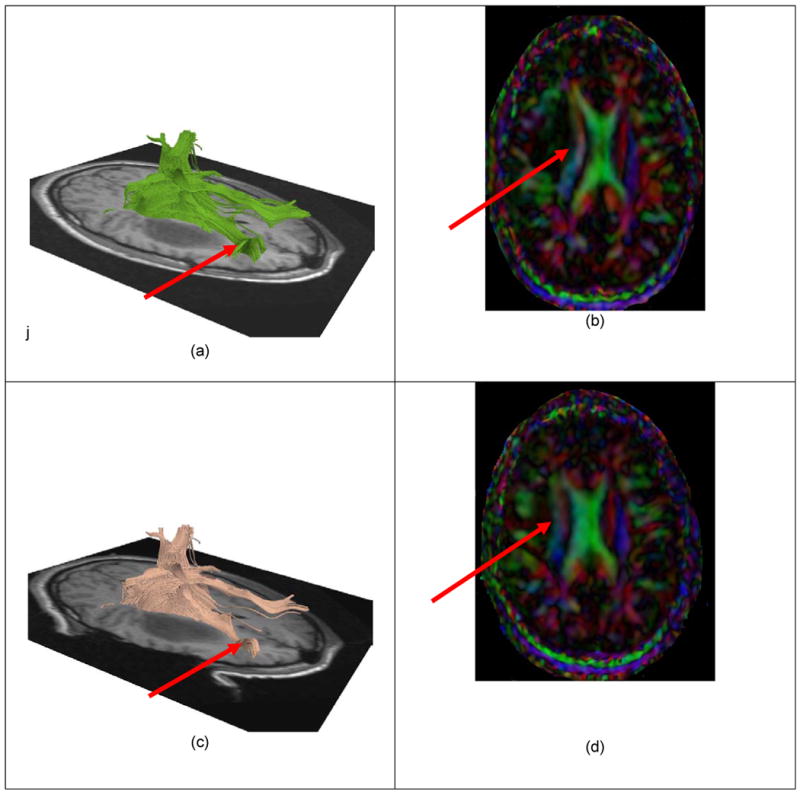
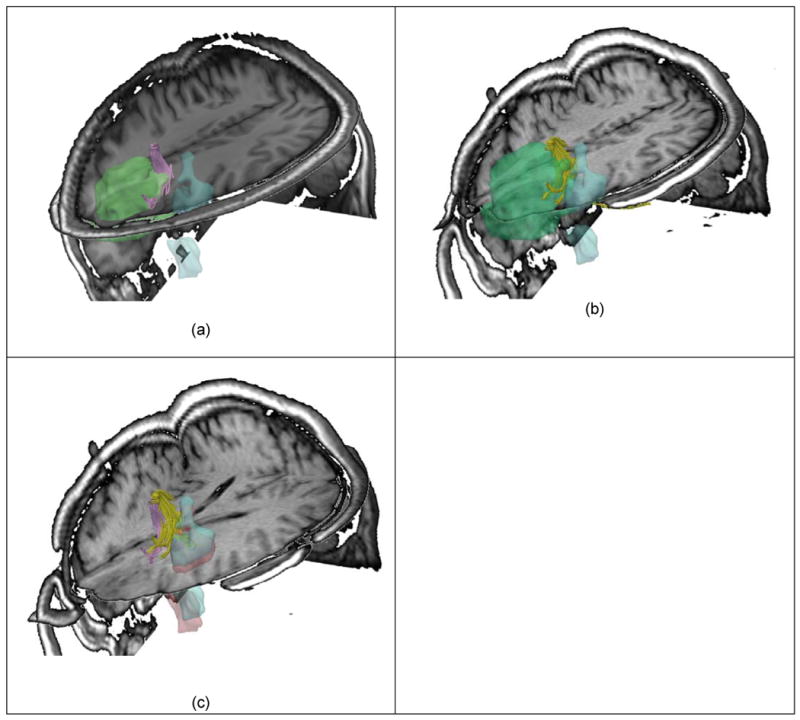
Conclusions: We were able to achieve intra-operative rigid and non-rigid registration of (1) pre-operative structural MRI with intra-operative T1w MRI; (2) pre-operative fMRI with intra-operative T1w MRI, and (3) pre-operative DT-MRI with intra-operative T1w MRI. The registration algorithms as implemented were sufficiently robust and rapid to meet the hard real-time constraints of intra-operative surgical decision making. The validation experiments demonstrate that we can accurately compensate for the deformation of the brain and thus can construct an augmented reality visualization to aid the surgeon.
Figures
References
-
- Alexander AL, Badie B, Field AS. Diffusion tensor MRI depicts white matter reorganization after surgery. Proceedings of the ISMRM 11th Scientific Meeting; Berkeley. International Society of Magnetic Resonance in Medicine; 2003.
-
- Arsigny V, Fillard P, Pennec X, Ayache N. Log-Euclidean Metrics for Fast and Simple Calculus on. Diffusion Tensors Magnetic Resonance in Medicine. 2006 Aug;56(2):411–421. - PubMed
-
- Atlas SW, Howard RS, Maldjian J, Alsop D, Detre JA, Listerud J, D'Esposito M, Judy KD, Zager E, Stecker M. Functional magnetic resonance imaging of regional brain activity in patients with intracerebral gliomas: Findings and implications for clinical management. Neurosurgery. 1996;38:329–338. - PubMed
-
- Audette MA. PhD. McGill University; 2003. Anatomical Surface Identification, Range-sensing and Registration for Characterizing Intrasurgical Brain Deformation.
-
- Audette MA, Siddiqi K, Ferrie FP, Peters TM. An integrated range-sensing, segmentation and registration framework for the characterization of intra-surgical brain deformations in image-guided surgery. Computer Vision and Image Understanding. 2003;89:226–251.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
