

Characterization of the severe asthma phenotype by the National Heart, Lung, and Blood Institute's Severe Asthma Research Program
- PMID: 17291857
- PMCID: PMC2837934
- DOI: 10.1016/j.jaci.2006.11.639
Characterization of the severe asthma phenotype by the National Heart, Lung, and Blood Institute's Severe Asthma Research Program
Abstract
Background: Severe asthma causes the majority of asthma morbidity. Understanding mechanisms that contribute to the development of severe disease is important.
Objective: The goal of the Severe Asthma Research Program is to identify and characterize subjects with severe asthma to understand pathophysiologic mechanisms in severe asthma.
Methods: We performed a comprehensive phenotypic characterization (questionnaires, atopy and pulmonary function testing, phlebotomy, exhaled nitric oxide) in subjects with severe and not severe asthma.
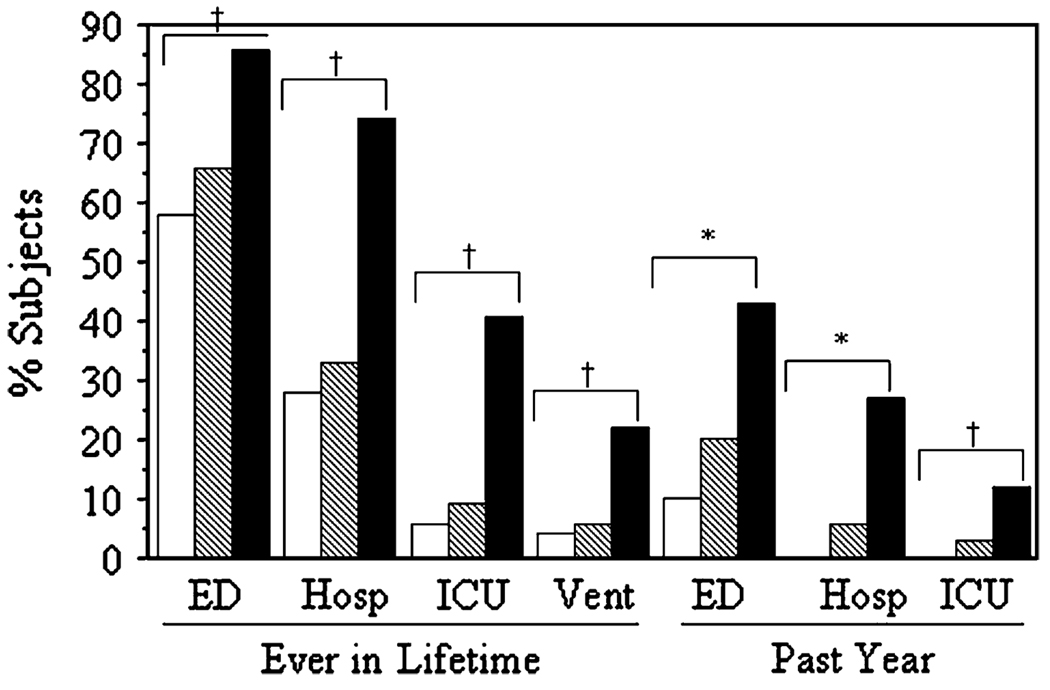
Results: A total of 438 subjects with asthma were studied (204 severe, 70 moderate, 164 mild). Severe subjects with asthma were older with longer disease duration (P < .0001), more daily symptoms, intense urgent health care utilization, sinusitis, and pneumonia (P < or = .0001). Lung function was lower in severe asthma with marked bronchodilator reversibility (P < .001). The severe group had less atopy by skin tests (P = .0007), but blood eosinophils, IgE, and exhaled nitric oxide levels did not differentiate disease severity. A reduced FEV(1), history of pneumonia, and fewer positive skin tests were risk factors for severe disease. Early disease onset (age < 12 years) in severe asthma was associated with longer disease duration (P < .0001) and more urgent health care, especially intensive care (P = .002). Later disease onset (age > or = 12 years) was associated with lower lung function and sinopulmonary infections (P < or = .02).
Conclusion: Severe asthma is characterized by abnormal lung function that is responsive to bronchodilators, a history of sinopulmonary infections, persistent symptoms, and increased health care utilization.
Clinical implications: Lung function abnormalities in severe asthma are reversible in most patients, and pneumonia is a risk factor for the development of severe disease.
Conflict of interest statement
Disclosure of potential conflict of interest: S. C. Erzurum has received grant support from Alair. L. Bacharier is on the speakers’ bureau for AstraZeneca, GlaxoSmithKline, Genentech, and Merck. W. J. Calhoun has consulting arrangements with Critical Therapeutics and Genentech. B. D. Levy has consulting arrangements with Critical Therapeutics. W. G. Teague is on the speakers’ bureau for Merck. W. W. Busse has consulting arrangements with Genentech/Novartis, Isis, GlaxoSmithKline, Altana, Wyeth, Pfizer, Dynavax, and Centocor, has received grant support from Novartis, Wyeth, Dynavax, Centocor, and GlaxoSmithKline, and is on the speakers’ bureau for GlaxoSmithKline, Novartis, Merck, and Astra-Zeneca. The rest of the authors have declared that they have no conflict of interest.
Figures
References
-
- Serra-Batlles J, Plaza V, Morejon E, Comella A, Brugues J. Costs of asthma according to the degree of severity. Eur Respir J. 1998;12:1322–1326. - PubMed
-
- Antonicelli L, Bucca C, Neri M, De Benedetto F, Sabbatani P, Bonifazi F, et al. Asthma severity and medical resource utilization. Eur Respir J. 2004;23:723–729. - PubMed
-
- Godard P, Chanez P, Siraudin L, Nicoloyannis N, Duru G. Costs of asthma are correlated with severity. Eur Respir J. 2002;19:61–67. - PubMed
-
- Busse WW, Banks-Schlegel S, Wenzel SE. Pathophysiology of severe asthma. J Allergy Clin Immunol. 2000;106:1033–1042. - PubMed
-
- Wenzel SE. Severe asthma in adults. Am J Respir Crit Care Med. 2005;172:149–160. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- HL69174/HL/NHLBI NIH HHS/United States
- R01 HL069155/HL/NHLBI NIH HHS/United States
- R01 HL069116/HL/NHLBI NIH HHS/United States
- HL69349/HL/NHLBI NIH HHS/United States
- R01 HL069349/HL/NHLBI NIH HHS/United States
- U10 HL109250/HL/NHLBI NIH HHS/United States
- M01 RR018390/RR/NCRR NIH HHS/United States
- R01 HL069130/HL/NHLBI NIH HHS/United States
- M01 RR03186/RR/NCRR NIH HHS/United States
- HL69130/HL/NHLBI NIH HHS/United States
- R01 HL069167/HL/NHLBI NIH HHS/United States
- HL69170/HL/NHLBI NIH HHS/United States
- HL69149/HL/NHLBI NIH HHS/United States
- HL69116/HL/NHLBI NIH HHS/United States
- R01 HL069174/HL/NHLBI NIH HHS/United States
- M01 RR003186/RR/NCRR NIH HHS/United States
- R01 HL069149/HL/NHLBI NIH HHS/United States
- R01 HL069170/HL/NHLBI NIH HHS/United States
- HL69167/HL/NHLBI NIH HHS/United States
- HL69155/HL/NHLBI NIH HHS/United States
- U10 HL109164/HL/NHLBI NIH HHS/United States
- M01 RR007122/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
